
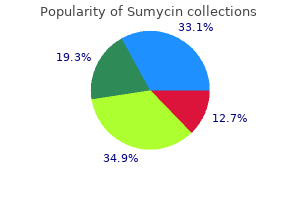
"Order sumycin australia, bacteria h pylori".
T. Pakwan, M.S., Ph.D.
Clinical Director, William Carey University College of Osteopathic Medicine
Anatomical studies by Ann Graybiel and her colleagues at the Massachusetts Institute of Technology have shown that regions of different cortical areas concerned with the hand (see Chapter 8) converge in specific rostrocaudal bands within the striatum; conversely, regions in the same corti- 420 Chapter Seventeen (A) Caudate Medium spiny neuron Medium spiny neuron (B) Dopaminergic neuron Local circuit neuron Cortical pyramidal neurons Globus pallidus or Substantia nigra pars reticulata neuron Medium spiny neuron Medium spiny neuron Putamen External Internal Globus pallidus Figure 17. The primary output of the medium spiny cells is to the globus pallidus and to the substantia nigra pars reticulata. Substantia nigra pars reticulata cal areas concerned with the leg converge in other striatal bands. These rostrocaudal bands therefore appear to be functional units concerned with the movement of particular body parts. Another study by the same group showed that the more extensively cortical areas are interconnected by corticocortical pathways, the greater the overlap in their projections to the striatum. A further indication of functional subdivision within the striatum is the spatial distribution of different types of medium spiny neurons. Although medium spiny neurons are distributed throughout the striatum, they occur in clusters of cells called "patches" or "striosomes," in a surrounding "matrix" of neurochemically distinct cells. Whereas the distinction between the patches and matrix was originally based only on differences in the types of neuropeptides contained by the medium spiny cells in the two regions, the cell types are now known to differ as well in the sources of their inputs from the cortex and in the destinations of their projections to other parts of the basal ganglia. For example, even though most cortical areas project to medium spiny neurons in both these compartments, limbic areas of the cortex (such as the cingulate gyrus; see Chapter 28) project more heavily to the patches, whereas motor and somatic sensory areas project preferentially to the neurons in the matrix. These differences in the connectivity of medium spiny neurons in the patches and matrix further support the conclusion that functionally distinct pathways project in parallel from the cortex to the striatum. Modulation of Movement by the Basal Ganglia 421 (A) Lateral view Primary visual cortex (B) Medial view Primary visual cortex Figure 17. The caudate, putamen, and ventral striatum receive cortical projections primarily from the association areas of the frontal, parietal, and temporal lobes. Primary auditory cortex the nature of the signals transmitted to the caudate and putamen from the cortex is not understood. It is known, however, that collateral axons of corticocortical, corticothalamic, and corticospinal pathways all form excitatory glutamatergic synapses on the dendritic spines of medium spiny neurons (see Figure 17. The arrangement of these cortical synapses is such that the number of contacts established between an individual cortical axon and a single medium spiny cell is very small, whereas the number of spiny neurons contacted by a single axon is extremely large. This divergence of axon terminals allows a single medium spiny neuron to integrate the influences of thousands of cortical cells. The medium spiny cells also receive noncortical inputs from interneurons, from the midline and intralaminar nuclei of the thalamus, and from brainstem aminergic nuclei. In contrast to the cortical inputs to the dendritic spines, the local circuit neuron and thalamic synapses are made on the dendritic shafts and close to the cell soma, where they can modulate the effectiveness of cortical synaptic activation arriving from the more distal dendrites. The aminergic inputs are dopaminergic and they originate in a subdivision of the substantia nigra called pars compacta because of its densely packed cells. The dopaminergic synapses are located on the base of the spine, in close proximity to the cortical synapses, where they more directly modulate cortical input (see Figure 17. As a result, inputs from both the cortex and the substantia nigra pars compacta are relatively far from the initial segment of the medium spiny neuron axon, where the nerve impulse is generated. Accordingly, the medium spiny neurons must simultaneously receive many excitatory inputs from cortical and nigral neurons to become active. When the medium spiny neurons do become active, their firing is associated with the occurrence of a movement. Extracellular recordings show that these neurons typically increase their rate of discharge just before an impending movement. Neurons in the putamen tend to discharge in anticipation of body movements, whereas caudate neurons fire prior to eye movements. These anticipatory discharges are evidently part of a movement selection process; in fact, they can precede the initiation of movement by as much as several seconds. Similar recordings have also shown that the discharges of some striatal neurons vary according to the location in space of the target of a movement, rather than with the starting position of the limb relative to the target. Thus, the activity of these cells may encode the decision to move toward the target, rather than simply the direction and amplitude of the actual movement necessary to reach the target. These nuclei are in turn the major sources of the output from the basal ganglia (Figure 17. The globus pallidus and substantia nigra pars reticulata have similar output functions. In fact, developmental studies show that pars reticulata is actually part of the globus pallidus, although the two eventually become separated by fibers of the internal capsule.
Cardiovascular System Radiographic Anatomy In general, the base of the heart is angled craniodorsally and lies at the second rib. The apex is directed in a caudoventral direction and lies between the fifth and sixth ribs (varies with species) (Figure 12. In mammals, various formulas for measuring the cardiac size from radiographs have proved inaccurate, and currently echocardiography is the most reliable method for assessing cardiac size and function. The lateral margins of a normal heart and liver in psittacine birds create an hourglass shape (Figure 12. In macaws, there is normally a ventrally directed kink between the heart and liver in the lateral view (Figure 12. Radiographic Evidence of Cardiac Disease Primary cardiac disease is rare, although congenital defects are occasionally detected on postmortem examination. Congenital and viral diseases should be considered in juvenile birds with cardiac murmurs, exercise intolerance and cardiomegaly. Pericardial effusion is recognized radiographically as a symmetrical, globoid enlargement of the cardiac silhouette and may occur in birds with chlamydiosis, polyomavirus, tuberculosis and neoplasia (Figure 12. Cardiomegaly may be caused by cardiomyopathy secondary to poxvirus (reported in macaws12), myxomatous valvular degeneration, endocarditis (particularly secondary to pododermatitis), hemochromatosis, chronic anemia and compression from extrinsic masses (see Chapter 27). Elongation of the heart shadow, loss of the caudal and cranial waists, loss of indentation at the junction between the heart and liver lobes and an increase in transatrial dimensions indicate an increase in cardiac size. Microcardia is associated with hypovolemia due to acute volume loss or endotoxic shock (see Figure 21. There is retraction of the heart from between the liver lobes, a more angular appearance to the cardiac shape and decreased transatrial size. Whatever the etiology, microcardia suggests a critical state, and appropriate volume replacement should be instituted immediately. Atherosclerosis with mineralization will result in prominence of the great vessels and may cause an increased density of the caudal lung field. Acute myocardial infarcts, syncope and seizures (perhaps due to hypoxemia) have been described in birds with atherosclerosis in the absence of radiographic lesions. Respiratory System Radiographic Anatomy the radiographic changes associated with respiratory disease are often subtle, and high quality radiographs are necessary to detect these lesions (Table 12. The trachea in toucans and mynah birds deviates ventrally at the level of the thoracic inlet (see Figure 47. Radiographically, the normal syrinx is difficult to visualize but lies between the second and third thoracic vertebrae in most birds (Figure 12. Lung parenchyma appears as a honeycombed structure with the majority of the air densities representing an end-on view of parabronchi (Figure 12. The bronchioles can be visualized as transverse, indistinct, linear structures on the ventrodorsal radiograph. Air bronchograms and atelectasis, which occur in mammals with pulmonary disease, do not occur in birds because of their unique lung anatomy (a network of inter-connecting tubules with the lungs adhered to the thoracic wall). Chronic nasal discharge, periorbital swelling and soft tissue masses are indications for radiographs of the nasal cavity and infraorbital sinus. Soft tissue swelling with osteolysis of the calvarium is often associated with osteomyelitis due to aspergillosis or mycobacteriosis. Air-filled swellings from distention of the cervicocephalic air sacs may be caused by infection, granulomas or idiopathic obstruction and should be differentiated from subcutaneous emphysema, which is more diffuse. Intraluminal soft tissue masses or undulating soft tissue plaques may be caused by bacteria, hypovitaminosis A, parasites, fungi, foreign body or neoplasm. A solitary mass in the syrinx may cause severe obstructive, open-mouthed dyspnea with no obvious radiographic changes. Superimposition of the great vessels, ribs and soft tissue over the syrinx compromises interpretation. A subtle increase in soft tissue in this region or fluid accumulation in the distal trachea suggests obstruction. Although contrast tracheography may help delineate some masses, tracheoscopy is less stressful to the patient and more definitive (Figure 12. Tracheal strictures secondary to trauma from fight-induced injuries or cuffed endotracheal tubes occasionally occur. Peritracheal masses may occur in the thoracic inlet due to thyroid enlargement secondary to goiter or neoplasm (Figure 12. With pulmonary disease, the normal honeycombed pulmonary parenchyma may be enhanced by parabronchial infiltration causing prominent ring shadows obliterated by filling of the parabronchial lumen with fluid or caseous exudate or replaced by neoplastic or granulomatous infiltrates (see Table 12.
Under these circumstances, the stabilized image actually disappears from perception within a few seconds! The blood vessels, which lie in front of the photoreceptor layer, cast a shadow on the underlying receptors. Although normally invisible, the vascular shadows can be seen by moving a source of light across the eye, a phenomenon first noted by J. This perception can be elicited with an ordinary penlight pressed gently against the lateral side of the closed eyelid. When the light is wiggled vigorously, a rich network of black blood vessel shadows appears against an orange background. The conventional interpretation of the rapid disappearance of stabilized images is retinal adaptation. Stabilizing the retinal image in one eye, for example, diminishes perception through the other eye, an effect known as interocular transfer. Although the explanation of these remarkable effects is not entirely clear, they emphasize the point that the visual system is designed to deal with novelty. Eye Movements and Sensor y Motor Integration 457 nerve carries axons that are responsible for pupillary constriction (see Chapter 11) from the nearby Edinger-Westphal nucleus. Thus, damage to the third nerve results in three characteristic deficits: impairment of eye movements, drooping of the eyelid (ptosis), and pupillary dilation. Types of Eye Movements and Their Functions There are four basic types of eye movements: saccades, smooth pursuit movements, vergence movements, and vestibulo-ocular movements. The functions of each type of eye movement are introduced here; in subsequent sections, the neural circuitry responsible for three of these types of movements is presented in more detail (see Chapters 13 and 18 for further discussion of neural circuitry underlying vestibulo-ocular movements). Saccades are rapid, ballistic movements of the eyes that abruptly change the point of fixation. They range in amplitude from the small movements made while reading, for example, to the much larger movements made while gazing around a room. Saccades can be elicited voluntarily, but occur reflexively whenever the eyes are open, even when fixated on a target (see Box A). The rapid eye movements that occur during an important phase of sleep (see Chapter 27) are also saccades. After the onset of a target for a saccade (in this example, the stimulus was the movement of an already fixated target), it takes about 200 milliseconds for eye movement to begin. During this delay, the position of the target with respect to the fovea is computed (that is, how far the eye has to move), and the difference between the initial and intended position, or "motor error" (see Chapter 18), is converted into a motor command that activates the extraocular muscles to move the eyes the correct distance in the appropriate direction. Saccadic eye movements are said to be ballistic because the saccade-generating system cannot respond to subsequent changes in the position of the target during the course of the eye movement. Smooth pursuit movements are much slower tracking movements of the eyes designed to keep a moving stimulus on the fovea. Such movements are under voluntary control in the sense that the observer can choose whether or not to track a moving stimulus (Figure 19. Most people who try to move their eyes in a smooth fashion without a moving target simply make a saccade. The smooth pursuit system can be tested by placing a subject inside a rotating cylinder with vertical stripes. There is then a quick saccade in the direction opposite to the movement, followed once again by smooth pursuit of a stripe. This alternating slow and fast movement of the eyes in response to such stimuli is called optokinetic nystagmus. Optokinetic nystagmus is a normal reflexive response of the eyes in response to large-scale movements of the visual scene and should not be confused with the pathological nystagmus that can result from certain kinds of brain injury (for example, damage to the vestibular system or the cerebellum; see Chapters 13 and 18). The red line indicates the position of a fixation target and the blue line the position of the fovea.
Syndromes
- Short stature
- Cancer
- Ear pain
- Weight gain
- Have a swollen abdomen (distention) that does not go away
- Ears that are prominent or that stick out may be treated for cosmetic reasons. During the newborn period, a small framework may be attached using tape or Steri-Strips. The child wears this framework for several months. Surgery to correct the ears cannot be done until the child is 5 years old.
- Fainting
- Fever
- Stroke
Snap traps baited with small quantities of ground meat are particularly effective. Snakes: Snakes will occasionally enter enclosures and consume small birds, but will rarely attack larger Psittaciformes. If an aviculturist is breeding small birds (canaries, finches, budgerigars, lovebirds) outdoors, the enclosure should be constructed with small wire or screen to prevent entry of snakes. Evaluating and Treating Flock Problems Emergency Care An experienced aviculturist is usually the first individual involved in providing emergency care to a sick or injured bird. The client should be well schooled in providing first aid and recognizing signs of illness that require veterinary intervention. The veterinarian should assist the aviculturist in preparing a first aid kit, in being prepared to provide post-examination nursing care and in having the necessary supplies to safely and effectively transport a sick bird (Table 2. Helping the aviculturist handle emergency problems will encourage the involvement of a veterinarian in the management of the collection (Figure 2. The aviculturist should visually evaluate each bird every day during routine feeding procedures. Fresh excrement should be evaluated for color, consistency and amount of feces, urine and urates (see Chapter 8). Managing Disease Outbreaks Rapid action early in a disease outbreak can prevent catastrophic losses. In an avicultural setting, maintaining flock health must be the priority, and containing an infectious agent, determining its source and implementing control procedures are mandatory. The more complete the medical examination (blood work, cultures, radiographs, endoscopy), the more likely the veterinarian is to be able to identify the problem and to make specific recommendations to prevent further illness in the flock. Sick birds should be immediately removed from the collection and a thorough diagnostic evaluation performed. If the bird dies, a complete necropsy with collection of representative tissues from all organ systems is critical. Many state diagnostic laboratories have free or relatively inexpensive fees for histopathology services. However, the period of time that elapses before these results can be obtained may allow an infectious agent to spread through a collection. When histopathology results are needed quickly, it is best to advise the aviculturist to spend the extra money and send samples to a private laboratory. Following an infectious disease outbreak, all materials that cannot be properly cleaned (eg, perches, wooden nest boxes) should be removed and destroyed. In any given medical situation, repairing management flaws and using biological control measures are superior to drug therapy. An easily and completely cleanable isolation area for new and sick birds should be available, and protocols should be established for managing this area. Evaluating Reproductive Failures Resident Bird Examination Annual examinations of all birds in a collection can be used to detect flock problems, establish and confirm the accuracy of identification systems and collect data that may lead to the removal of unproductive individuals. The efficacy of husbandry practices and the plane of nutrition can be determined by assessing the physical condition of the birds. The veterinarian working in unison with the aviculturist may be able to determine correctable physical, hormonal, nutritional, behavioral and psychological causes of reproductive failure. A review of the potential health problems identified during the previous breeding season and appropriate testing of nonproductive birds can provide information that is critical to identifying the source of a problem (see Chapter 29). Estimating the age of a bird may be helpful in understanding reproductive failure. Birds purchased as part of an entire collection that is being dissolved may be less risky. Dealing with birds that are to be removed from a collection can challenge the ethics of the veterinarian. Euthanasia of valuable birds due to poor reproductive success or due to poorly understood medical problems (such as cloacal papillomatosis) is unacceptable to many people. Resale of these birds without full disclosure of their problems is equally unacceptable and can strain the client/veterinarian relationship. It is never advisable for the same veterinarian to represent both the buyer and the seller in a bird transaction.