
"Cheap 5 mg montelukast fast delivery, asthma 9 year old".
R. Keldron, M.A.S., M.D.
Professor, Western University of Health Sciences
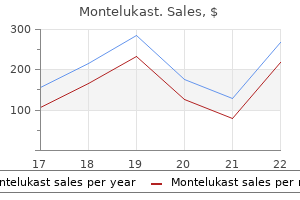
The disease burden was particularly high in India and Indonesia, with a prevalence of 43. Other recent studies show that prevalence amongst trans women living in urban cities or states is even higher than national prevalence levels. As shown in Figure 2, data are available for Jakarta, Indonesia, Maharastra, India, and amongst hijra sex workers in Larkana, Pakistan. For example, in this region, this is the case in Cambodia, Indonesia, and Pakistan. But they have no access to preventive measures, testing, or knowledge and information about symptoms and treatment. In Pakistan, the only available comparisons are between male sex workers and hijra sex workers 37 3 3. The first is assuming that trans men primarily engage in sex with cisgender women (often lesbians, who are assumed to be low risk) and the couple are assumed to use low-risk sexual practices. The second assumption is that, whatever their sexual orientation, the types of sex trans men have involve few risks. Yet trans men inhabit a wide range of sexual orientations and sexual behaviours, and may have cisgender or trans partners. These are often referred to by trans men as "rear" and "frontal" sex, respectively. As a result, trans men may not have sufficient knowledge or power to negotiate safe sex (Sevelius, 2009). Trans men who enter a gay male community after transitioning often face new sexual negotiations. They may choose to compromise safety rather than risk rejection because of a strong desire to have their masculinity affirmed by a gay male partner (Rowniak et al. Projects and programmes such as these can also contribute to addressing current data gaps by adding to the body of available surveillance data. Working with the clinic also makes it easier to provide direct referrals to other treatment, care, and support services. But most of our members go out at night and the desk may not be reaching everyone. Its staff, peer educators and volunteers are all trans women-who often use local terms like kathoey or sao praphet song. Over the last 10 years, Sisters has worked with almost 5,000 trans women across different communities, including sex workers, cabaret showgirls and youth. Peer educators are also available to visit trans women at home to provide counselling and information on hormone therapy and gender-affirming surgeries. By providing this range of services in a welcoming space, the clinic aims to reduce the stigma and discrimination trans people face when moving between different health services. Each regional peer educator has a project phone to coordinate the clients into one place and then fetch them in a bus so they can access services, including treatment. The clinic provides this additional support only to trans women because of the high incidence and severity of abuse they face in trying to reach the clinic. Stigma and discrimination were frequent and trans women were not being served, so the project developed a peer navigator programme. Now the project sensitises all of the healthcare workers throughout the city and includes trans women in the health worker trainings. Figure 5: Gonorrhoea and chlamydia prevalence amongst trans women, 20092012 50 40 Gonorrhea Chlamydia Percentage 30 20 10 0 Vientienne and Savannakhet Lao (2012) National Kota Bandung Indonesia (2013) In the Indian city of Pune, the genital ulcer disease prevalence was 15. Fear of being judged by health providers may discourage some trans people from seeking treatment for substance use disorders, including dependence. There is minimal research on these issues-particularly on whether access to gender-affirming health services can reduce over-reliance on drugs or alcohol. In Asia and the Pacific, there are very limited quantitative data on alcohol and drug use amongst trans people. Anecdotal evidence suggests that drug use may be an emerging health issue for trans men in Asia. In the five countries in Asia where data are available (Bangladesh, Indonesia, Malaysia, Pakistan, and the Philippines46), between 0. Behavioral Surveillance Survey 200607; (2) Ministry of Health Republic of Indonesia. For this reason, research also has focused on the extent to which trans people, including sex workers, have used drugs or alcohol before sex.
Attention focused internally toward the lower abdominals will disrupt a normal bracing maneuver by the entire lower trunk and degrade the learning process of the transfer or lift. An exercise set up with movement goals that accomplish the desire recruitment pattern will improve coordination more efficiently. Some level of internal awareness of body position and abdominal tightening may be necessary, but directing full attention internally toward specific muscles can disrupt the execution of automated skills and can have a degrading effect on the learning of new skills (NcNevin et al. Hollowing is an appropriate technique for motor learning for isolation of the TrA, but not necessarily for normal stability or function. Bracing is the more natural and functional approach for the abdominal contribution toward dynamic stability. In some cases an initial approach directed internally toward isolation of the TrA with hollowing type exercises may be a necessary first step in a progression. An approach of bracing should, however, be the emphasis and eventual progression for all spinal stabilization training. Exercises can be designed to naturally recruit the deep anterior muscles without an internal focus but through an external resistance that naturally recruits these muscles. With the focus more on performance of an activity that naturally recruits certain fiber directions, motor learning can address functional movements and occur more quickly. Care should be taken to avoid directing exercise too much toward learning specific rehabilitation exercises versus learning more functional movements. The weight of the organs on the abdomen wall provides feedback for contraction of the TrA muscle. Whether TrA hallowing or abdominal bracing is preferred, practice can involve many other functional motions such as rolling transfers and lifting. Iliacus and psoas activation is not consistent with spinal movement but primarily hip flexion (Juker et al. The iliacus has been shown to stabilize the pelvis in contralateral hip extension during standing, while the psoas is selectively involved in contralateral trunk loading situations, requiring stabilization of the spine in the frontal plane (Andersson et al. The iliacus also produces hip flexion but working alone without the psoas creates an anterior pelvic tilt, forcing the spine into lumbar extension. The psoas provides minimal spinal segment stability and shear stiffness but only in the presence of hip flexion torque (McGill 1998). In some cases, excessive tone is present in the hip flexors, preventing normal movement and creating secondary pain from muscle guarding. An elevation in tone of the hip flexors may be directly related to pain and spinal facilitation or related to compensation for weak lower abdominals. These muscles often test short with muscle length tests but this is largely due to elevated resting tone. Directly training the hip flexors (as above) may be helpful with acute guarding to increase circulation and reduce tone but if they are over active, compensating for lower abdominal weakness, than a combination of down training the hip flexors while up-training the lower abdominals is most efficient. Reducing hip flexor contribution to cranial trunk flexion (sit ups) has largely focused on the position of the hip. The more common approach is to flex the hip to shorten the hip flexors in attempt to make them actively insufficient. The position of the hips and lower quarter is not as important as whether an extensor pattern or flexor pattern is facilitated in the lower limbs during the movement (Janda 1996). Hooking the feet to stabilize the lower limbs recruits a flexor pattern of ankle dorsiflexors, knee flexors and hip flexors (psoas and iliacus). Sit-ups performed in this position emphasize the hip flexors rather than the lower abdominals. Creating an extensor pattern would more effectively inhibit the hip flexors to allow for trunk flexion to be performed to a greater extent by the lower abdominals. Performing cranial flexion with the hips in a flexed position attempts to reduce recruitment of the hip flexors during the motion. This approach is largely ineffective and will continue to facilitate the hip flexors. The movement also emphasizes the cranial portion of the rectus abdominus, which has little contribution to spinal stabilization. Any block of the lower limbs in supine, incline or sitting will facilitate a flexor pattern increasing emphasis of the hip flexors and reducing emphasis of the abdominals.
Immediate Family Members means your Spouse or Domestic Partner and their children, including adopted children or step-children; legal guardians or wards; siblings or siblings-in-law; parents or parents-in-law; grandparents or grandchildren; aunts or uncles; nieces or nephews. Your insurance automatically terminates on the earliest of the following: · the termination date of the policy · the expiration of the period for which required premium has been paid for you · the date on which you no longer meet the eligibility criteria as an Insured Person · the date on which the Company pays out 100% of the benefit amount If I charge multiple Common Carrier fares on my Account for myself and Immediate Family Members, does this benefit apply separately to each person? The benefit covers physical loss or damage of Checked Baggage and/or Carry-On Baggage and personal property in the baggage 18 Questions? Some of the documentation the Company may request includes, but is not limited to: · a completed claim form · a copy of the travel itinerary · written confirmation that the claim was filed with the Common Carrier · a copy of the credit card statement that shows the charge for the Common Carrier fare · a copy of the settlement or denial from the Common Carrier · copies of receipts for the purchase of replacement items over twenty-five ($25. You must provide a written claim notice within twenty (20) days after the occurrence or commencement of any loss or damage covered by this policy or as soon as reasonably possible. This written description should include information detailing the occurrence, type, and extent of the loss for which the claim is made. You need to send the Company complete Proof of Loss within ninety (90) days from the date of loss or as soon as reasonably possible. Please note that failure to provide Proof of Loss within these time frames will not invalidate or reduce any otherwise valid claim if notice is given as soon as is reasonably possible, and in no event later than one (1) year after the ninety (90) day deadline to submit Proof of Loss, except in cases where the claimant lacks legal capacity. Spouse your husband or wife who is recognized as such by the laws of the jurisdiction in which you reside. War hostilities following a formal declaration of war by a governmental authority; in the absence of a formal declaration of war by a governmental authority, armed, open and continuous hostilities between two countries or armed, open and continuous hostilities between two factions, each in control of territory or claiming jurisdiction over the geographic area of hostility. General Provisions: the terms We, Us and Our below refer to Federal Insurance Company. No such action may be brought after three (3) years from the time written Proof of Loss is required to be furnished. Carry-On Baggage suitcases or other containers specifically designated for carrying personal property, which are carried on board a Common Carrier by an Insured Person. As a handy reference guide, please read this and keep it in a safe place with your other insurance documents. Policy # 9907-28-44 Federal Insurance Company, a member insurer of the Chubb Group of Insurance Companies, is the underwriter of this insurance policy and is solely responsible for its administration and claims. Rewards program manager, Tour Operator, Travel Agency, or Travel Supplier the Company will reimburse the Insured Person ($. Reimbursement is subject to the following: · Cancellation provisions in effect at the time the Travel Supplier is notified of a cancellation. Immediate Family Member means your Spouse or Domestic Partner and their children, including adopted children or step-children; legal guardians or wards; siblings or siblings-in-law; parents or parents-in-law; grandparents or grandchildren; aunts or uncles; nieces or nephews. It does not apply to a Covered Loss caused directly or indirectly from: · travel arrangements canceled or changed by a Common Carrier, Tour Operator, or any Travel Agency unless the cancellation is the result of severe weather or an organized strike affecting public transportation · change in plans, financial circumstances, and any business or contractual obligations applying to you, your Traveling Companion, your Immediate Family Member, an Immediate Family Member of your Traveling Companion · a Pre-existing Condition 22 Questions? If a Trip Interruption occurs, the Company will reimburse you for up to the maximum Benefit Amount of five thousand ($5,000. This benefit does not apply to a Covered Loss caused directly or indirectly from the Insured Person or Traveling Companion: · traveling against the advice of a Physician · traveling while on a waiting list for specified medical treatment · traveling for the purpose of obtaining medical treatment; or traveling in the third trimester (seventh month or after) of pregnancy · traveling with a Pre-Existing Condition · commission or attempted commission of any illegal act including but not limited to any felony · being engaged in or participating in a motorized vehicular race or speed contest · participating in any professional sporting activity for which the Insured Person received a salary or prize money · traveling or flying on any aircraft engaged in flight on a rocket propelled or rocket launched aircraft · suicide, attempted suicide or intentionally self-inflicted injury Additionally, this insurance does not apply to any Accident, Accidental Bodily Injury or loss caused by or resulting from, directly or indirectly: 1) Common Carrier caused delays, unless they are as a result of an organized strike that affects public transportation; 2) travel arrangements canceled or changed by a Common Carrier, Tour Operator, or any travel agent unless the cancellation is the result of severe weather or an organized strike affecting public transportation; 3) change in plans, financial circumstances and any business or contractual obligations of the Insured Person, Traveling Companion, Immediate Family Member of the Insured Person or Immediate Family Member of the Traveling Companion; 4) any occurrence while the Insured Person is incarcerated; 5) when: a) the United States of America has imposed any trade or economic sanctions prohibiting insurance of any Accident, Accidental Bodily Injury or loss; or b) there is any other legal prohibition against providing insurance for any Accident, Accidental Bodily Injury or loss; or 6) a declared or undeclared War the Trip Interruption benefit is excess over any travel insurance purchased by the Insured Person for the same Covered Trip or other indemnity by the airline, cruise line, railroad, station authority, occupancy provider available to the Insured Person. Immediate Family Member, means your Spouse or Domestic Partner and their children, including adopted children or step-children; legal guardians or wards; siblings or siblings-in-law; parents or parents-in-law; grandparents or grandchildren; aunts or uncles; nieces or nephews. Some of the prepaid travel arrangements that are eligible for reimbursement include, but are not limited to , airline tickets, train tickets, bus tickets, prepaid tours, hotels, and rental cars. If I charge multiple travel arrangements for myself and Immediate Family Members, do the benefits apply to each person? Yes, each traveler is eligible to receive the primary benefit up to the Trip Cancellation & Trip Interruption Maximum Limit of Insurance per Occurrence. What is the Trip Cancellation & Trip Interruption Maximum Limit of Insurance per Occurrence? If a Covered Loss results in Benefit Amounts becoming payable, which when totaled, exceed the applicable Trip Cancellation & Trip Interruption Maximum Limit of Insurance per Occurrence, then the Trip Cancellation & Trip Interruption Maximum Limit of Insurance per Occurrence will be divided proportionally among the Insured Persons, based on each applicable Benefit Amount. As long as you have charged the travel arrangements to your card, the Company will pay the corresponding benefit regardless of whether you are traveling with them, as subject to the terms and conditions of this description of coverage. Definitions Accident or Accidental a sudden, unforeseen, and unexpected event which: · happens by chance · arises from a source external to an Insured Person · is independent of illness, disease or other bodily malfunction or medical or surgical treatment thereof Will the benefits be payable to me? You may use the Credit Card to purchase, hire, rent or lease property or services Dependent your Dependent Child, Spouse or Domestic Partner Dependent Child your unmarried child, Dependent on you for maintenance and support, under the age of 24, under the age of 25 if enrolled as a full-time student at an Institution of Higher Learning or classified as an Incapacitated Dependent Child Domestic Partner a person designated by you who is registered as a Domestic Partner or legal equivalent under the laws of the governing jurisdiction or who is at least 18 years of age and competent to enter into a contract; is not related to you by blood; has exclusively lived with you for at least 12 consecutive months prior to the date of enrollment; is not legally married or separated and as of the date of enrollment has with you at least 2 of the following financial arrangements: a joint mortgage or lease, a joint bank Account, joint title to or ownership of a motor vehicle or status as a joint lessee on a motor vehicle lease or a joint Credit Card Account with a financial institution. Spouse your husband or wife who is recognized as such by the laws of the jurisdiction in which you reside Travel Agency an entity with whom travel arrangements were made for an Insured Person and purchased by you using your Account Tour Operator an entity which organizes travel components into packaged arrangements for sale directly to the travelling public Travel Supplier a Tour Operator, occupancy provider, cruise line, airline, railroad or other Common Carriers Traveling Companion an individual who has made advanced arrangements with you to travel together for all or part of the Covered Trip War hostilities following a formal declaration of war by a governmental authority; in the absence of a formal declaration of war by a governmental authority, armed, open and continuous 28 Questions?
Angle-closure glaucoma develops when the iris blocks the drainage network of the eye, as shown in this illustration. This occurs in patients who are susceptible to this condition because they are farsighted or have cataracts. Angle-closure glaucoma is more common among people over age 50 because the incidence of cataracts increases with age. The symptoms of acute angle-closure glaucoma are severe ocular pain, blurred vision, halos around lights, headache, nausea, and vomiting. The slide shows the associated external ocular signs: injected conjunctiva, hazy cornea, and pupil fixed and mid-dilated. Whenever acute angleclosure glaucoma is suspected, the patient should be referred immediately for an ophthalmic evaluation to measure the intraocular pressure and initiate medical therapy. When anti-cholinergic medications indicate glaucoma as a potential side effect, the warning usually is related to the risk of causing angle-closure glaucoma in susceptible individuals. This hole provides an alternate path for fluid to reach the anterior chamber and the drainage network of the eye. In the Framingham Eye Study, the incidence of cataracts causing a decrease in vision to 20/30 or less increased from 18% between 65 and 74 years of age to 46% between 75 and 85. Damage can occur as a result of chronic exposure to sunlight, age, diabetes, steroid use, smoking, trauma, and previous surgery. Patients are first aware of a disturbance of vision and then a diminution in vision. The primary care physician may be asked to assist in the preoperative evaluation of patients to determine their risk of complications when undergoing cataract surgery. Cataract surgery is now almost always performed under local anesthesia (where retrobulbar or peribulbar injection is performed) or topical anesthesia (where anesthetic drops or topical gels are instilled sometimes in conjunction with intraocular administration of anesthetic solution). Cataract surgery and other ophthalmic eye operations performed under local anesthesia are relatively low risk, but arrhythmias can develop with the anesthetic injection for globe manipulation. Because patients are asked to lie supine under sterile sheets for up to an hour, those with pulmonary disease may need to have their pulmonary function and medications optimized prior to surgery. This allows the implantation of an artificial intraocular lens within the capsular bag, as shown in this illustration. In addition, leaving the capsular bag behind reduces the risk of retinal detachment and macular edema following surgery. Cataract surgery is one of the most successful surgical procedures performed today: 90% of patients achieve vision of 20/40 or better. The infrequent complications include infection, glaucoma, and retinal swelling or detachment. However, in about 15% of patients, the remaining lens capsule becomes opaque following cataract surgery and causes decreased vision. Fortunately, vision in such patients can be improved by making an opening in this remaining capsule with a laser. Patients often misunderstand this procedure and erroneously believe that initial cataract surgery can be performed solely with a laser. Because diabetic retinopathy is an important cause of visual loss, the Academy offers a slide program solely on this subject, Diabetes and Eye Disease, so it will be covered only briefly here. Macular edema is caused by leakage from microaneurysms and other damaged vasculature. Note the yellowish hard exudates, composed of lipid and other serum precipitates, in the macula. Although it is usually thought of as a cause of moderate visual loss, macular edema can cause blindness. A multicenter randomized clinical trial performed by the Early Treatment Diabetic Retinopathy Study Research Group has shown that laser surgery is effective in reducing the risk of moderate visual loss from macular edema. Proliferative diabetic retinopathy, characterized by neovascularization, is a response to ischemia caused by capillary dropout. It is recommended that patients with type I diabetes have an annual eye exam beginning 5 years after diagnosis. Good glycemic control should be recommended to all patients with diabetic retinopathy to reduce the risk of macular edema and proliferative diabetic retinopathy, as well as other problems. Good glycemic control in type I diabetes mellitus may involve the use of multiple daily insulin injections. In addition, controlling blood pressure and lipid levels not only are critical for general medical care in patients with diabetes but also may reduce the risk of retinal abnormalities from diabetes.