
"Purchase serpina 60 caps, anxiety side effects".
X. Marius, M.A., M.D., Ph.D.
Vice Chair, Oregon Health & Science University School of Medicine
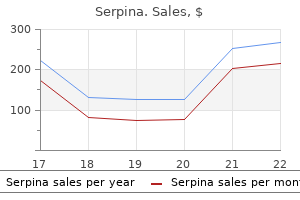
Every year, the seasonal influenza vaccine protects against three or four different strains of the virus, based on predictions experts believe will be the most virulent strains affecting humans. See Centers for Disease Control and Prevention, Selecting the Viruses in the Seasonal Influenza (Flu) Vaccine: Questions and Answers (2014). Barry, the Great Influenza: the Story of the Deadliest Pandemic in History 452 (rev. It resulted in fewer deaths compared to other influenza pandemics, with nearly 20,000 deaths in confirmed cases worldwide. At any time, any influenza viral strain could evolve into a more or less hazardous form. Unlike seasonal influenza, there will be no vaccine available to the public for a pandemic viral strain early in a pandemic, and vaccines produced to thwart yearly seasonal influenza outbreaks will be ineffective. While an influenza pandemic on the scale of the 1918 pandemic has not occurred, public health officials acknowledge that an outbreak of this magnitude is likely to occur, and emergency preparedness plans must be developed to address this foreseeable event. An influenza pandemic will likely result in an overwhelming number of patients who are critically ill, commonly presenting symptoms such as high fever, lower respiratory tract infection, abdominal pain, diarrhea, and vomiting. Pneumonia, acute respiratory distress syndrome, and multi-organ failure are probable for many influenza patients and a ventilator, a device that facilitates breathing for patients experiencing respiratory failure, will be needed. Bird-to-human transmission has occurred, mostly via direct human contact with the secretions and/or excretions of infected poultry. See World Health Organization, Avian influenza: significance of mutations in the H5N1 virus (2006). However, the virus is adept at mutating and can gain the ability to spread among humans after initial bird-to-human transmission. Highly pathogenic avian influenza is associated with a range of illnesses, from conjunctivitis only, to serious respiratory illness with multiple organ failure and can lead to death. Bed-side ventilators are stationary machines while transport ventilators can be moved with a patient. Furthermore, it may be difficult to adapt 26 Chapter 1: Adult Guidelines Currently, New York State has 7,241 ventilators available in acute care facilities, of which approximately 2% are restricted for neonatal patients only; 8% are suitable for pediatric patients only; 50% could support either an adult or pediatric patient ("dual-use" ventilators); and nearly 41% are for adult patients only. During non-emergency, normal conditions, there is an 85% utilization rate of ventilators in acute care facilities, leaving only 15% of ventilators available. For example, as the pandemic spreads, hospitals should limit the non-critical use of ventilators. Elective procedures should be canceled and/or postponed during the period of emergency. As a pandemic stretches from days to weeks, facilities will require a review system for procedures that decrease morbidity or mortality, but are not of an emergency nature. In addition, outpatient procedures that require a back-up option of hospital admission and ventilator therapy if complications arise may be limited. In addition to ventilators, facilities should address surge capacity for other important components of the health care system, including staff and medical equipment and supplies. Staffing issues are critical, because personnel are the most valuable resource in any health care facility. Staff members may become ill, leave work to care for loved ones, or decline to serve from fear of contagion. Furthermore, the stockpiling of protective personnel equipment, including masks and gloves, is a critical planning responsibility for facilities. Without adequate protective measures, facilities may undermine their capacity to provide adequate staffing during a public health emergency. Surge capacity could also be assisted by activating systems for sharing information about the number and severity of influenza cases, equipment availability, and staffing shortages throughout hospital systems and regional networks. For instance, not all facilities may be equipped to care for infants who need ventilator treatment; clinicians need rapid access to information about where such support is available. Of the 7,241 ventilators in New York State, 124 ventilators can only support neonates, 731 can only support pediatric patients, 2,717 can support either children or adults, and 3,669 can only support adult patients. New York State Department of Health, Office of Health Emergency Preparedness Program, Critical Assets Survey, September 2015. Estimates of the Possible Impact of Pandemic Influenza in New York State the Department of Health has examined moderate and severe pandemic influenza outbreak scenarios to estimate the potential impact and ventilator need at acute care facilities during a pandemic.
For other lung conditions, a detailed description of symptoms/diagnosis, surgical intervention, and medications should be provided. The applicant should describe the condition to include, dates, symptoms, and treatment, and provide medical reports to assist in the certification decision-making process. These reports should include: operative reports of coronary intervention to include the original cardiac catheterization report, stress tests, worksheets, and original tracings (or a legible copy). Part 67 provides that, for all classes of medical certificates, an established medical history or clinical diagnosis of myocardial infarction, angina pectoris, cardiac valve replacement, permanent cardiac pacemaker implantation, heart replacement, or coronary heart disease that has required treatment or, if untreated, that has been symptomatic or clinically significant, is cause for denial. Issuance of a medical certificate to an applicant with high blood pressure may depend on the current blood pressure levels and whether the applicant is taking anti-hypertensive medication. If a surgical procedure was done, the applicant must provide operative and pathology reports. If a 38 Guide for Aviation Medical Examiners procedure was done, the applicant must provide the report and pathology reports. A medical history or clinical diagnosis of diabetes mellitus requiring insulin or other hypoglycemic drugs for control are disqualifying. The applicant should provide history and treatment, pertinent medical records, current status report and medication. An established diagnosis of epilepsy, a transient loss of control of nervous system function(s), or a disturbance of consciousness is a basis for denial no matter how remote the history. Like all other conditions of aeromedical concern, the history surrounding the event is crucial. Substance dependence; or failed a drug test ever; or substance abuse or use of illegal substance in the last 2 years. A careful history concerning the nature of the sickness, frequency and need for medication is indicated when the applicant responds affirmatively to this item. Because motion sickness varies with the nature of the stimulus, it is most helpful to know if the problem has occurred in flight or under similar circumstances. It is helpful to know the circumstances surrounding the discharge, including dates, and whether the individual is receiving disability compensation. The fact that the applicant is receiving disability benefits does not necessarily mean that the application should be denied. For each admission, the applicant should list the dates, diagnoses, duration, treatment, name of the attending physician, and complete address of the hospital or clinic. The applicant must name the charge for which convicted and the date of the conviction(s), and copies of court documents (if available). If additional records, tests, or specialty reports are necessary in order to make a certification decision, the applicant should so be advised. The applicant must report any disability benefits received, regardless of source or amount. Visits to Health Professional Within Last 3 Years the applicant should list all visits in the last 3 years to a physician, physician assistant, nurse practitioner, psychologist, clinical social worker, or substance abuse specialist for treatment, examination, or medical/mental evaluation. The applicant should list visits for counseling only if related to a personal substance abuse or psychiatric condition. The applicant should give the name, date, address, and type of health professional consulted and briefly state the reason for the consultation. Multiple visits to one health professional for the same condition may be aggregated on one line. Although there are no medical standards for height, exceptionally short individuals may not be able to effectively reach all flight controls and must fly specially modified aircraft. Since height is commonly measured in centimeters, divide height in centimeters by 100 to obtain height in meters. The head and neck should be examined to determine the presence of any significant defects such as: a. The external ear is seldom a major problem in the medical certification of applicants. Discharge or granulation tissue may be the only observable indication of perforation. Mobility should be demonstrated by watching the drum through the otoscope during a valsalva maneuver. Pathology of the middle ear may be demonstrated by changes in the appearance and mobility of the tympanic membrane. An upper respiratory infection greatly increases the risk of aerotitis media with pain, deafness, tinnitus, and vertigo due to lessened aeration of the middle ear from eustachian tube dysfunction.
After the administration of midazolam, the child is observed for at least 2 hours to recover fully from the sedation. Documentation should be provided for the dosage, method and time of administration, and the reaction to the drug. Informing the parents that the investigation will cause pain despite measures to relieve pain and anxiety in the child is important, as is informing the child that the investigation may be somewhat difficult for him or her but it will be done fast. The child will in almost all cases cry during the examination and will need soothing after it is completed. Evaluation for anal incontinence and constipation means two needle insertions (with standard concentric needle vs. Thus, despite discomfort in connection with the investigation, it is possible to carry out a neurophysiologic evaluation of sphincter dysfunction in children. Gutierrez C, Marco A, Nogales A, Tebar R: Total and segmental colonic transit time and anorectal manometry in children with chronic idiopathic constipation. Karlbom U, Edebol Eeg-Olofsson K, Graf W, et al: Paradoxical puborectalis contraction is associated with impaired rectal evacuation. Page numbers followed by the letter f refer to figures; those followed by the letter t refer to tables. Alpha coma, 115, 115f, 313 in head-injured child, 377 Alpha rhythm, 12 posterior frequency, 109 suppression of, due to hyponatremia, 333, 333f variants of, 91 slow, 110 Alpha squeak phenomenon, 109, 110f Alsin gene, in juvenile amyotrophic lateral sclerosis, 575 Alternating current, 8 Amacrine cells, of retina, 206 Ambiguous sleep. Brachial neuritis, idiopathic, 598 Brachial plexopathy, postnatal, 595-600 hereditary neuropathies in, 597-598, 597f, 598b idiopathic neuropathy in, 598 neoplastic, 599, 599b osteomyelitis-related, 596-597, 596b, 596f pressure palsies in, 598-599 pseudoparesis in, 600 thoracic outlet syndrome in, 599-600, 599b traumatic, 599 Brachial plexus anatomy of, 582, 583f-585f, 584 components of, 582 cords of, 584 lesions of. Idiopathic anhidrosis, chronic, 703 Idiopathic autoimmune neuropathy, acute, 698 outcome of, 699 Idiopathic-related partial epilepsies, 233-238. Incus, 182, 183f vibration of, 187-188, 187f Infant benign myoclonic epilepsy in, 239 born to drug-dependent mother, 314 early epileptic encephalopathy in, 244, 245f facial palsies in. Lennox-Gastaut syndrome, 242-243 slow-wave patterns in, 125, 127f Lesch-Nyhan syndrome, 340-341 Leukemia, acute lymphoblastic. See also Average montage; Bipolar montage; Referential montage; Transverse montage. Nucleotide metabolism, disorders of, 757 Nutritional deficiencies, polyneuropathies associated with, 672b, 673 Nyquist theorem, 22, 23f O Obstetric palsy. Poliomyelitis, 573-574 neurophysiologic testing for, 574 postimmunization, neuromuscular crisis in, 766-767 Polygraphic data, scoring of, in sleep-wake disorders, 391-392, 394f-395f, 394t, 395t Polyneuritis cranialis, facial diplegia due to , 536, 537f Polyneuropathy(ies), 645-673 axonal, 664-668 acute acquired, 664-665 chronic genetically-determined, 666-668 electrophysiology of, 664 clinical history of, 646 critical illness, 656, 769, 773 differential diagnosis of, 656b differentiating features of, 772t demyelinating acute, 652-657 chronic inflammatory, 663-664. A history of multiple impacts to the head (eg, via contact sports, military service, domestic violence, head banging, among others), including concussion and subconcussion 2. No other neurologic disorder that accounts for all of the clinical features, although it can be comorbid with other psychiatric and neurodegenerative conditions 3. Behavioral symptoms primarily characterized by aggressive and explosive behaviors 2. Mood dysfunction characterized by depression and related symptoms (eg, hopelessness, depression) 3. Cognitive difficulties that involve cognitive decline and impaired cognitive test performance (ie, 1. Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic encephalopathy syndrome. Normal amyloid beta levels and elevated p-tau/ tau ratios in the cerebrospinal fluid22 2. This work was also supported by unrestricted gifts from the Andlinger Foundation, the World Wrestling Entertainment and the National Football League. Furthermore, prospective studies are needed to precisely define the clinical manifestations of the disease and the role of factors such as cognitive reserve, lifestyle choice, and comorbid medical conditions in the clinical expression of the disease. Cognitive effects of one season of head impacts in a cohort of collegiate contact sport athletes. Chronic traumatic encephalopathy: a potential late effect of sportrelated concussive and subconcussive head trauma. Neuropathological observations in a case of autism presenting with self-injury behavior. Chronic traumatic encephalopathy in blast-exposed military veterans and a blast neurotrauma mouse model.
While the risk of transmission increases with advancing gestational age, the severity of fetal sequelae is more pronounced the earlier in gestation the fetus is affected. The value of routine toxoplasmosis screening programs is debated in the United States but generally accepted in other countries. In countries such as France where pregnant women are universally screened and treated, infected offspring are reported to have primarily mild disease and rarely severe disease. Studies published since 2007 support treatment of toxoplasmosis during pregnancy in an effort to decrease vertical transmission and reduce the severity of clinical signs in the offspring. Spiramcyn is not teratogenic, does not treat infection in the fetus and is primarily indicated for fetal prophylaxis. Pyrimethamine should not be used in the first trimester because of teratogenicity concerns. While there are limited data on atovaquone safety in humans, preclinical studies have not demonstrated toxicity. Maintenance therapy should be provided, using the same indications as for non-pregnant women. Outbreak of central-nervous-system toxoplasmosis in western Europe and North America. Central-nervous-system toxoplasmosis in homosexual men and parenteral drug abusers. Use of a clinical laboratory database to estimate Toxoplasma seroprevalence among human immunodeficiency virus-infected patients. Toxoplasma gondii infection in the United States, 1999 2004, decline from the prior decade. Incidence and risk factors for toxoplasmic encephalitis in human immunodeficiency virus-infected patients before and during the highly active antiretroviral therapy era. Pyrimethamine for primary prophylaxis of toxoplasmic encephalitis in patients with human immunodeficiency virus infection: a double-blind, randomized trial. Risk factors for Toxoplasma gondii infection in mothers of infants with congenital toxoplasmosis: Implications for prenatal management and screening. Use of the peroxidase-antiperoxidase method to demonstrate toxoplasma in formalin fixed, paraffin embedded tissue sections. A randomized trial of three antipneumocystis agents in patients with advanced human immunodeficiency virus infection. A randomized trial comparing pyrimethamine plus clindamycin to pyrimethamine plus sulfadiazine. Treatment of central nervous system toxoplasmosis with pyrimethamine/ sulfadiazine combination in 35 patients with the acquired immunodeficiency syndrome. Folinic acid supplements to pyrimethamine-sulfadiazine for Toxoplasma encephalitis are associated with better outcome. Cotrimoxazole for treatment of cerebral toxoplasmosis: an observational cohort study during 1994-2006. Clarithromycin-minocycline combination as salvage therapy for toxoplasmosis in patients infected with human immunodeficiency virus. The immune inflammatory reconstitution syndrome and central nervous system toxoplasmosis. Plasma pharmacokinetics of sulfadiazine administered twice daily versus four times daily are similar in human immunodeficiency virus-infected patients. Maintenance therapy with cotrimoxazole for toxoplasmic encephalitis in the era of highly active antiretroviral therapy. Low incidence of congenital toxoplasmosis in children born to women infected with human immunodeficiency virus. Congenital toxoplasmosis occurring in infants perinatally infected with human immunodeficiency virus 1. Mother-to-child transmission of toxoplasmosis: risk estimates for clinical counselling.