
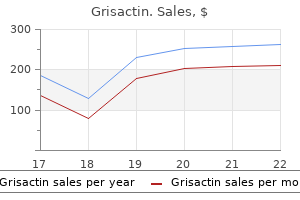
"Order generic grisactin on line, treatment plans for substance abuse".
Y. Sigmor, M.A., M.D., Ph.D.
Clinical Director, Eastern Virginia Medical School
In lead V2, the chest lead, the electrode is in a field of very negative potential, which occurs in patients with an anterior lesion. C) the right axis deviation in this patient has to occur because of a change in muscle mass in the right ventricle, which occurs in pulmonary valve stenosis. Aortic valve insufficiency and systemic hypertension will cause a left axis shift. A) this patient has an acute anterior infarction in the left ventricle of the heart. This diagnosis can be determined by plotting the currents of injury from the different leads (see figure below). The limb leads are used to determine whether the infarction is coming from the left or right side of the ventricle and from the base or inferior part of the ventricle. The chest leads are used to determine whether it is an anterior or posterior infarct. E) During the T-P interval in a patient with a damaged ventricle, the only area depolarized is the damaged muscle. At the J point the entire ventricle is depolarized in a patient with a damaged cardiac muscle or in a patient with a normal cardiac muscle. The area of the heart that is damaged will not repolarize but remains depolarized at all times. Pulmonary hypertension increases the ventricular mass on the right side of the heart, which gives a right axis deviation. D) In the figure below, the current of injury is plotted at the bottom of the graph. The negative end of the vector points to where the current of injury originated, which is in the apex of the ventricle. Systemic hypertension, aortic valve stenosis, and aortic valve regurgitation cause hypertrophy of the left ventricle and thus a leftward shift in the mean electrical axis. Therefore, the diagnosis that fits with these characteristics is a right bundle branch block. E) this patient has a difference in the atrial rate of 100 and in the ventricular rate of 25. The 25 rate in the ventricles is indicative of a rhythm starting in the Purkinje fibers. A-V block is occurring, but it comes and goes, which is only fulfilled by Stokes-Adams syndrome. The atria exhibit circus movements, and atrial volume is often increased, causing the atrial fibrillation. A) Circus movements occur in ventricular muscle, particularly in persons with a dilated heart or decreases in conduction velocity. High extracellular potassium and sympathetic stimulation, not parasympathetic stimulation, increase the tendency for circus movements. A longer refractory period tends to prevent circus movements of the heart, because when the impulses travel around the heart and contact the area of ventricular muscle that has a longer refractory period, the action potential stops at this point. D) When a patient has no P waves and a low heart rate, it is likely that the impulse leaving the sinus node is totally blocked before entering the atrial muscle, which is called sinoatrial block. The ventricles pick up the new rhythm, usually initiated in the A-V node at this point, which results in a heart rate of 40 to 60 per minute. B) By definition, first-degree A-V heart block occurs when the P-R interval exceeds a value of 0. Once again notice that the heart rate is irregular because of the inability of the impulses to quickly pass through the A-V node because of its refractory period. B) A dilated heart increases the risk of occurrence of ventricular fibrillation because of an increase in the likelihood of circus movements. Also, if the conduction velocity decreases, it will take a longer period for the impulse to travel around the heart, which decreases the risk of ventricular fibrillation. Exposure of the heart to 60-cycle alternating current or epinephrine administration increases the irritability of the heart. If the refractory period is long, the likelihood of re-entrant type of pathways decreases, because when the impulse travels around the heart, the ventricles remain in a refractory period. D) An inverted P wave occurs in patients with a premature contraction originating in the A-V junction. E) the term "paroxysmal" means that the heart rate becomes rapid in paroxysms, with the paroxysm beginning suddenly and lasting for a few seconds, a few minutes, a few hours, or much longer.
Patients who survive a lesion above C7 usually remain dependent on others for daily care. Sparing of the C7 segment retains elbow and wrist extension and enables transfer from wheelchair to bed, providing a degree of independence. Recovery may theoretically occur as the roots regenerate, perhaps only after many months delay. The posterior spinal arteries: usually arise from the posterior inferior cerebellar arteries and form a plexus on the posterior surface of the spinal cord. The anterior spinal artery: branches from each vertebral artery unite to form a single vessel lying in the median fissure of the spinal cord. Basilar artery Posterior inferior cerebellar artery Vertebral artery Vertebral artery Both anterior and posterior spinal arteries run the length of the spinal cord and receive anastomotic vessels. The plexus of the posterior spinal artery is joined by approximately 12 unpaired radicular feeding arteries. This rich collateral circulation protects the posterior part of the spinal cord from vascular disease. The anterior spinal artery has a much less efficient collateral supply and is thus more vulnerable to the effects of vascular disease. Cervical arteries arise from vertebral and subclavian vessels, form plexuses and supply the cervical and upper thoracic cord. This level of the spinal cord is liable to damage during hypertension watershed area. Artery of Adamkiewicz, the largest radicular artery, supplies the low thoracic and lumbar cord. It usually arises at T9L2 level and is on the left side in 70% of the population. Sacral arteries arise from the hypogastric artery and supply the sacral cord and cauda equina. Anterior spinal artery territory Penetrating branches anterior and part of posterior grey matter. Posterior spinal artery Posterior radicular artery Most radicular vessels only supply the root. On average 12 posterior radicular branches and 8 anterior radicular branches supply the spinal cord. When infarction occurs in the anterior spinal artery territory it is often a consequence of disease in the vessels of origin of the segmental arteries, i. Characteristic features include: Radicular pain at onset Sudden para/quadraplegia days Flaccid limbs spastic days Areflexia hyper-reflexia and extensor plantar responses Sensory loss to pain and temperature up to the level of cord damage Preserved vibration and joint position sensation (dorsal columns supplied by the posterior spinal arteries) Urinary retention When only penetrating branches are involved, long tract damage may be selective and sensory loss may be minor. Spinal cord ischaemia due to aortic atheroma evolves slowly and preferentially affects anterior horn cells. Posterior spinal artery syndrome this is rare as white matter structures are less vulnerable to ischaemia. Clinical features: Loss of tendon reflexes/motor weakness Loss of joint position sense. Site Cervical: uncommon site (~15%) Arises from the anterior spinal artery and usually lies within the cord substance (intramedullary). Most are dural arterio-venous fistula where the branches of the radicular artery drain directly into the dural venous plexus; in others the radicular artery drains into the dorsal spinal venous plexus. Treatment should prevent progression and may well improve a gait or bladder disturbance. Surgery It is important to identify and divide the feeding vessel and excise the shunt. Operative risk for most dural A-V fistula is low and excision provides an alternative to embolisation. Staged pre-operative embolisation may help, but in some, a conservative approach may be appropriate. Spinal Epidural and Subdural Haematomas: these may present with a rapid onset of paraplegia. Urgent decompression is required after correcting any coagulation deficit, without waiting for spinal angiography. Pathological examination of the haematoma may reveal angiomatous tissue; in other patients, there is no evident cause. In most patients, the meningeal covering ruptures and the spinal cord and roots lie exposed to the air myelodysplasia.
For mothers who have been in labour recession of the foetal presenting part and disappearance of foetal heart sounds suggest rupture of the uterus. Once rupture of the uterus has been ruled out then treatment for abruptio placentae should be instituted. This is done when vaginal delivery is evaluated as imminent and feasible · Indications for abdominal delivery; Caesarian section, hysterotomy - intrauterine foetal death with severe uterine bleeding - severe degree of placental abruption with a viable foetus - haemorrhage severe enough that it jeopardizes life of mother - any incidental complication of labour · Postpartum; continue oxytocin for about 2 hours. Placenta Praevia the management of placenta praevia depends on gestation, extent of bleeding and clinical findings. The decision follows after evaluation, complete examination of maternal and foetal status. Palpitations, body oedema, cough, easy fatigability, evidence of heart enlargement, murmurs, thrills, left parasternal heave, raised jugular venous pressure. Management - Supportive · Bed rest · Haematinic supplementation · Treat intercurrent infections · Avoid undue physical and emotional stress · Regular urine analysis and culture · Ensure dental hygiene · Regular U/E. Management - Pharmacologic · Digitalization is indicated in imminent and overt cardiac failure, if not previously on digoxin · Continue maintenance therapy with digoxin, frusemide · Continue prophylactic benzathine penicillin monthly. Suitable methods include minilaparotomy, tubal ligation under local anaesthesia, vasectomy, barrier methods, progesterone only agents. Clinical Features Overt diabetes If not already diagnosed the symptoms include: polydipsia, polyuria, weight loss, blurred vision, lethargy. Historical risk factors include: Previous gestational diabetes, family history of diabetes, previous macrosomic infant, previous unexplained still birth, polyhydramnios, obesity, advanced maternal age. Complications of diabetes include Chronic hypertension and nephropathy, pregnancy-induced hypertension, foetal macrosomia, intrauterine growth retardation, polyhydramnios, foetus distress, hypoglycaemia. Patient Education · Pre-pregnancy counselling: Achieve optimum glucose control before pregnancy to minimize foetal complications in diabetic pregnancy · Family planning: Advise on a small family. The following table provides guidelines on drugs which are considered safe or relatively safe in pregnancy, drugs which should be used with caution and only when necessary, and drugs which are contraindicated. The clinical features of malaria in pregnancy depend, to a large extent, on the immune status of the woman, which in turn is determined by her previous exposure to malaria. Clinical Features 229 Non-immune (women from endemic area): High risk of maternal perinatal mortality. Acute febrile illness; severe haemolytic anaemia; hypoglycaemia; coma/convulsions; pulmonary oedema. One of the dangers of malaria in these settings is that it is not detected or suspected. Antimalarials should form part of the case management of all women with severe anaemia who are from endemic irrespective of whether they have a 230 fever or a positive blood slide [see 18. This may however be negative in a woman from endemic areas, despite placental parasitisation. Management - Supportive · Check blood sugar regularly as hypoglycaemia is a common problem in women with severe disease · Correct dehydration · Evacuation if incomplete/inevitable abortion · Delivery if foetal death or established labour Management - Pharmacologic · For clinical disease it is essential to use the most effective antimalarial drug available. Dextrose use helps avoid quinine- induced maternal hypoglycaemia · Other drugs that can be used for treatment in pregnancy in the second and third trimesters are artemisinin derivatives. If travel is not avoidable they should take special precautions in order to prevent being bitten such as using mosquito repellents and an insecticide treated bednet. Mostly twin pregnancy but others may be encountered, triplets, etc and these may be associated with use of fertility drugs. Multiple pregnancy generally 231 carries a much higher risk (antenatal, intrapartum and postpartum) than a singleton. Foetal heart rates at two different areas with a difference of 15 beats per minute. Investigations · X-ray at 34-36 weeks · Other investigations as for routine antenatal care Definitive diagnosis can be made by ultrasonography. Management - Intrapartum · Mode of delivery determined by presentation of first twin: - if cephalic allow vaginal delivery - any other presentation or anomaly, then Caesarean section · Vaginal Delivery: - monitor as per normal labour (refer to normal labour and delivery) - after delivery of first twin the lie and presentation of the second foetus is determined. Otherwise do a Caesarean section to expedite delivery at shortest possible interval which should be the overall goal. Patient Education · Family planning · Early ante-natal visit at subsequent pregnancies. Hypertension being defined as a blood pressure of 140/90 or higher on more than 2 occasions of about 6 hours apart.
This leads ed injuredthe dose theprotein or drugs being used may activation and patients the hepatic the and coagulation abnormalities. This to be dose of dose of or drug being used may need be h as hypotension, secondarybe withheld. All of these complications need or a of the pain threshold threshold thatthe patient more sensitive to pain, to pain, ing resetting of to be considered in this makes the patient more sensitive tting of the painthe pain that makes the patient more sensitive to pain, isease. Analgesia should always be ethe as theis notedandbe painful to for weeks to "wind-up". In ownersIn situations where months and owners he animal animalto virus ispersistavoid infurthermonths andIn situations whereweeks to oon environment isbecan to be hardy further "wind-up". Not is going and performed advised type of surgery) analgesics should always eir going to be should performed. Wheneverdilute bleach suspected the animal should vely to prevent prevent wind-up from occurring. A foot Administrationof gowns and and personnel should the gowns and ration of Analgesics tration of Analgesics of Analgesics algesicsbeto thebath should be initially to ensure adequate blood levels are hould beshould intravenously initially to initially to ensure adequateunit. The subcutaneous route should be avoided avoided in dehydrated or y rapidly as possible. The subcutaneous route should be avoided in dehydrated or nimals animals sinceof the drugthetoo unpredictable. Intramuscular injections fusingsince uptake of uptakeTests drug is too unpredictable. Intramuscular injections Diagnostic of too ade presumptively usedbeon inis onlyand termof when no other route isis routeand age of the animal. On presentation a primary Opioids along anestheticsvary from stable toagonists be given via the via the long beinglocalstatus can from -2 and -2 On can alsoto death from along with close to death and septic shock. Epiduralswhile a complete history anesthesia; ction injection or via a Epidurals patient are not be delayed in theisunder anesthesia; a complete history is ection or via catheter. Epidurals usually usually are administered critical patient while however, resuscitation should administered under ctice practicebe rapidly obtained from the placedbeunder sedationsedationfrom local withboth injectionsinjections and cathetersplaced placed underobtained and the owner to allow treatment to be sion both injections and catheterspermission should be rapidly and local ce should both and catheters can be owner under sedation and be obtained. Instead can be can to allow treatment to local ding on the location of the tip of an epidural catheter effective analgesiaanalgesia can nding on the location location of antip of an epidural catheter effective can a. Depending on the of the tip the epidural catheter effective analgesia can started. Usually morphine or hydromorphone are ver, however, many other as well as -2completeagonists havesurveyused completed once the primary survey is ever, many other secondary survey, or agonists have been used via the is via the omplete physical opioids opioids completed -2 physical examination, ed; many otherA examination, is as well as oncehaveprimary been the opioids as well as -2 agonists the been used via is oute. The esthesia isis desired then and anesthetics are instituted addition to the nesthesia desiredis desired then local anestheticsat ininfused the the signs ion If anesthesia indicated. Patients may respiratory depression, paralysis, hypothermia, urinary pneumonia (aspiration or bradycardia, hypotension, have concurrent pressure. The abdomenauscultationavoided avoidedanesthetics should be palpated and ausculted. A rectal exam should be performed and the following should be evaluated: consistency of stool, evidence of blood, and dilation of the rectum. A Doppler ultrasonic blood flow detector or an oscillometric device can be used; however, the Doppler is preferred since it allows the clinician to evaluate perfusion or flow as well as blood pressure. Diagnostic tests are required frequently in order to determine the extent of the disease and to confirm the diagnosis. Resuscitation of the critical patient should not be delayed while tests are being performed unless those tests are required to guide resuscitation. Many of these puppies are hypoglycemic and require a bolus of dextrose followed immediately by dextrose supplementation in the fluids. A complete blood count with microscopic evaluation of a blood smear for the differential is essential as leukopenia is associated with a more guarded prognosis. A lymphopenia of <1000/ul within 48h of admission was found in one study to be a negative prognostic indicator.
These objects should be readily familiar to most patients and come from different "categories". For example, I use "piano" "baseball bat" and the color "blue" (These are my unique 3 objects. Make sure that the patient can accurately and immediately repeat the objects and tell them that you will be asking them to recall them in a few minutes. If the patient cannot immediately accurately recall each of the three objects, then this is a deficit of registration (not short-term memory) which is really a task of concentration and not of short-term memory. Assuming registration is intact, if the patient cannot recall one or more of the objects after several minutes, then give them a clue. Language While there are many different types of memory which can be better settled with neurocognitive testing, we will focus on short-term memory and long-term memory here. Long-term memory is the most ingrained with any sort of encephalopathy and is therefore, the most resilient and "last to go". Asking historical questions about where the patient went to high school, their birth date, their wedding anniversary, the names of their parents, etc. Therefore, one should perform tasks of Alertness and Orientation as well as tasks of Concentration before moving on to the rest of the Mental Status exam. Once again, try to quantify the deficit by having the patient try to name easier objects (such as a watch or thumb) then move on to more difficult names (such as a watch band or index finger). As with memory, language is complex and best "broken down" through neurocognitive testing. For the purposes of a general neurological examination however, we will stick to "expressive language", "receptive language", and "repetition". This is essentially the left hemisphere for right handed individuals and may be the right hemisphere, left hemisphere or have bilateral representation for left handed individuals. Patients with "aphasias" will have difficulty not only with spoken language, but also with reading, writing, sign language, and facial expressions or hand gestures that are used to communicate meaning. Dysarthria does not localize to the language areas of the brain but may be secondary to motor functions in the frontal lobe, deep sub-cortical basal ganglia regions, brainstem or their connections. Good ways to test expressive language include asking a patient to perform a multi-step task. Remember that a 3-step task is more difficult than a one-step task and that midline tasks (such as "open your mouth") are easier than appendicular task (such as "show me the thumb on your left hand"). Having the patient perform a task that they need to read is also helpful in distinguishing alexia from aphasia. The result is a fluent aphasia, where the patient rambles on in a incoherent fashion. Therefore, a good screening task for all of these areas is to ask the patient to repeat a complex sentence. I always use "today is a sunny day in the city of New Orleans", though other phrases such as "there are no ifs, ands, or buts about it" are commonly used. Make sure the sentence is somewhat complex and if the patient cannot repeat it accurately, move towards an easier sentence. The cranial nerve exam reflects the function of the brainstem and can help to co-localize long track findings. Cranial Nerves this nerve is rarely tested except in cases of closed head injury where shearing forces can sever branches coming off the olfactory nerves as they transverse the skull base at the cribiform plate. There is a direct air communication in the superior nasal passageways so that it is difficult to isolate deficits of the olfactory nerve to the right or left side exclusively. Noxious stimulation (such as smelling ammonium salts) actually irritates the nasal mucosa which is supplied by the Maxillary division of the Trigeminal Nerve. Therefore, to test olfactory function, the patient should be asked to distinguish between smells such as coffee and cinnamon or other spices. The Optic Chiasm sends fibres reflecting visual input from the lateral visual fields from each eye to the contralateral Lateral Geniculate Nucleus.