
Isabel Filges, M.D.
- Medical Genetics
- University Hospital Basel
- Switzerland
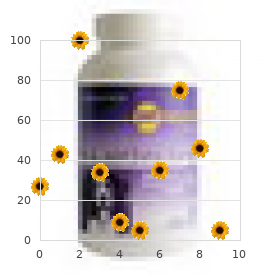
About 15% to 20% of cases happen in youngsters youthful than 1 year of age anxiety pill 027 discount effexor xr 37.5mg amex, most often in affiliation with a congenital diaphragmatic defect anxiety attack symptoms yahoo purchase generic effexor xr on-line. Hematemesis is uncommon however could additionally be as a outcome of anxiety symptoms going crazy order effexor xr on line amex an esophageal tear or gastric mucosal ischemia anxiety for no reason generic effexor xr 37.5 mg on line. The mixture of ache anxiety symptoms keep coming back purchase effexor xr american express, unproductive retching anxiety blood pressure effexor xr 37.5mg free shipping, and lack of ability to pass a nasogastric tube is known as Borchardt triad. The surgeon must have a low threshold for making this prognosis in a patient that presents with this symptom complicated. Chronic gastric volvulus is associated with mild and nonspecific symptoms like dysphagia, epigastric discomfort or fullness, bloating, and heartburn, significantly after meals. Using fluoroscopy, the endoscope is advanced to form an alpha loop in the proximal stomach. This method is most often used in chronic gastric volvulus with out signs of ischemia. Surgery for gastric volvulus could additionally be performed by open or minimally invasive methods. In current years, minimally invasive restore has turn out to be the gold standard for restore of chronic volvulus. Insufflation of the stomach may not be hemodynamically tolerated in a critically unwell patient. Combined endoscopic and laparoscopic restore or simple endoscopic gastropexy by placement of a percutaneous gastrostomy tube has been reported. If the patient is clinically secure, the surgeon may elect to deal with the underlying explanation for the volvulus. It is uncommon to have a gastric volvulus in the absence of an related paraesophageal hernia. In the lateral belly wall, there are layers of muscle tissue that together with intervening fascia present support. These muscle tissue travel at oblique angles to one another and therefore handle forces in varied planes, affording larger assist than if they were parallel to one another. In the central stomach, the cumbersome rectus abdominis muscles present a barrier to herniation. Abdominal wall hernias happen in areas the place these muscular tissues and fascial layers are attenuated, and the hernias can be congenital or acquired. In the groin, an area vulnerable to herniation is bounded by the rectus abdominis muscle medially, the inguinal ligament laterally, and the pubic ramus inferiorly; the aponeurosis of the transversus abdominis muscle supplies the deep layer. Upright posture causes intra-abdominal pressure to be constantly directed to this space. The processus vaginalis may persist in 12% to 20% of adults, additional predisposing to hernia formation. Therefore, oblique inguinal hernias journey with the spermatic wire (or spherical ligament) and are discovered lateral to the inferior epigastric vessels, whereas direct hernias are found within the flooring of the inguinal canal-an space supported only by the weak transversalis fascia-and are medial to the inferior epigastric vessels. Femoral hernias move through the opening related to the femoral artery and vein. However, it is necessary to accurately diagnose femoral hernias because they can be mistaken for lymph nodes within the groin. Misinterpreting an incarcerated loop of bowel in a femoral defect as a lymph node can lead to fine-needle aspiration of the mass and bowel harm. The omentum, colon, small bowel, and bladder are the commonest contents of groin hernias, although the appendix, Meckel diverticulum, fallopian tube, and ovary have been reported to herniate. In this case, the affected person can have strangulation of the bowel with out evidence of bowel obstruction, which is often present when bowel is incarcerated in a hernia. B, Barium examination displaying that the larger curvature and lesser curvature of the stomach are reversed in position (upside-down stomach). C, Twisting of the gastric folds at the point of torsion is famous on this endoscopic view of a gastric volvulus. The external indirect muscle has been omitted, and the spermatic cord (the round ligament in women) is retracted. Spigelian hernia happens by way of defects within the fused aponeurosis of the internal oblique and transverse abdominal muscles. Direct inguinal hernia occurs through defects in the transversalis fascia in Hesselbach triangle. Femoral hernia happens inferior to the inguinal ligament and medial to the femoral vein and femoral artery. Epidemiology the lifetime threat of groin hernia requiring restore is 27% for males and 3% for girls, with restore seen most often in children beneath age 5 and adults older than 70. In males, direct inguinal hernias account for about 30% and femoral hernias for about 1%. In women, about 25% of groin hernias requiring repair are femoral, and the incidence will increase with age. Congenital hernias are extra frequent in males as a outcome of they symbolize a patent processus vaginalis. These pediatric hernias are commonly bilateral, and pediatric surgeons are taught to always evaluate the contralateral side. Clinical Features, Diagnosis, and Complications Many groin hernias are asymptomatic. The most common symptom is a mass in the inguinal or femoral space that enlarges when the patient stands or strains. In a Richter-type hernia, pain from bowel strangulation might occur with out symptoms of obstruction, as just one wall of the gut is concerned in the hernia. Richter hernias are commonest in the femoral space, additional complicating the prognosis. Femoral hernias are most typical in ladies, in whom clinicians may have a lower stage of suspicion for hernia than in males. A examine by the American College of Surgeons has shown that males with minimally symptomatic groin hernias could be safely watched. Only 2 of the 364 patients in the watchful waiting arm of the research developed issues associated to their hernia in 4. This suggests that minimally symptomatic sufferers could be watched safely and have their hernia repaired when symptoms increase. The patient should be watched intently to guarantee useless bowel has not been reduced into the peritoneal cavity, a state of affairs that can trigger peritonitis and demise. Repair of the hernia should occur inside that same hospitalization, unless there are medical points that justify a delay. Groin hernias could be repaired utilizing numerous methods, including open or minimally invasively, with or without mesh, and are a source of ongoing debate for surgeons. However, several studies have shown a decreased recurrence fee with the use of mesh resulting in tension-free repairs, each for open and laparoscopic repairs. There are 2 key elements to profitable hernia repair: (1) high ligation of the hernia sac, which treats the direct defect, and (2) repair of the floor of the canal, which treats the indirect defect. These repairs contain strategy to the inguinal canal through a small incision parallel to the inguinal ligament and centered over the internal inguinal ring. Dissection is sustained through the external indirect muscle, exposing the inner inguinal ring. The wire structures are then isolated and explored completely to determine an oblique hernia sac, which is ligated and transected. The floor of Hesselbach triangle is then reinforced and strengthened by apposing the lateral border of the rectus abdominis aponeurosis to the inguinal ligament (Bassini or Shouldice repair) or to Cooper ligament (McVay repair). Mesh plug repairs have also been developed and appear to have outcomes just like other repairs. The mesh causes fibroblast ingrowth and scarring that leads to strengthening of the ground of the inguinal canal. Mesh repairs have the advantage of being considerably less complicated to perform than tissue repairs and have less pressure, much less acute pain, and a decreased fee of recurrence. The largest and most recent study was performed by the Veterans Cooperative group. Patients who had their hernias repaired laparoscopically had much less ache initially and returned to work 1 day ahead of those that had open repair. Meta-analyses of open versus laparoscopic repair have advised that laparoscopic repair causes less ache, but recurrence price is greater, as is the chance of complications. Those with recurrent or bilateral hernias can be thought of for laparoscopic repair, which may be performed successfully in experienced palms. The mesh is positioned and the flap is reattached to forestall the mesh from being involved with bowel. Post-Surgery Complications and Recurrence Elective groin hernia restore is secure, and critical problems are unusual. Minor acute issues embrace acute urinary retention, seroma, hematoma, and infection. This may be handled by native nerve block, desensitization therapy, and neurectomy. The threat of recurrence is expounded to situations that result in tissue deterioration, corresponding to malnutrition, liver or renal failure, glucocorticoid therapy, and malignancies. As talked about, recurrence charges are greater with laparoscopic hernia repair than with open herniorrhaphy. Overall, recurrence charges are greater after tissue repairs than after tension-free mesh repairs. Diastasis recti is a separation of the rectus abdominis muscular tissues and not using a defect in the abdominal fascia and may be demonstrated as a midline defect exaggerated by a Valsalva maneuver. Incisional hernias embody postlaparotomy hernias, parastomal hernias, and trocar-site hernias. Etiology and Pathophysiology Incisional hernias are brought on by patient- and surgery-related components. It is extra widespread for hernias to develop after a vertical midline incision than after a transverse incision. Development of a postoperative wound infection can lead to a better incidence of hernia formation. By putting these intentional hernias throughout the rectus muscle somewhat than lateral to the rectus, or by using mesh to reinforce the world, the danger of parastomal hernia can be decreased. The price of hernia formation is related to the scale of the trocar used (trocars > 10 mm in diameter are more generally associated with hernia formation), size of surgery, obesity, and advancing age. Inguinal Hernias and Colorectal Cancer Screening Some practitioners suggest that patients aged 50 years or older with inguinal hernias be screened for colorectal neoplasms earlier than hernia repair. One older prospective study utilizing versatile sigmoidoscopy to display primarily middle-aged or aged males with inguinal hernias reported the prevalence of colorectal polyps to be 26% and the prevalence of colorectal cancers to be 3. In such patients, it could be advisable to defer the examination till after hernia restore. When followed carefully over an extended period, up to 20% of sufferers can be discovered to develop a hernia. For example, the smallest fascial defect is created inside the rectus sheath, somewhat than lateral to it. The use of organic mesh in primary stoma placement may reduce the incidence of subsequent hernia formation, but this routine use of mesh is controversial, and a multicenter randomized controlled trial is planned to tackle this. Conversely, the risk of postoperative urinary retention after hernia restore is increased by prostatic hyperplasia, and older male sufferers with any symptoms of prostate illness should be counseled on the risk of urinary retention after hernia repair. It is important that the prostatism is dealt with medically previous to elective hernia repair. This will avoid urinary retention postoperatively that could be painful and prolong size of stay. If elective inguinal hernia repair and transurethral prostatic resection are required, some surgeons would think about performing these procedures concurrently,129,a hundred thirty however extra frequently, issues about infection of mesh lead to sequential surgical procedure. This shrinkage can improve the house between the bowel wall and fascia, facilitating hernia formation. Clinical Features, Diagnosis, and Complications Incisional hernias could cause persistent stomach discomfort. Because the fascial defect of incisional hernias is often large, strangulation is uncommon even with incarceration. Reduced ability to voluntarily improve intra-abdominal pressure interferes with defecation and urination. Surgeons need to watch out about reducing and repairing these large hernias, as a result of the acute increase in stomach strain can result in pulmonary failure and reduced venous return, resulting in an efficient belly compartment syndrome. Incarceration and strangulation of bowel may happen within the parastomal defect, presenting as a bowel obstruction. Trocar website hernias are especially challenging to diagnose, as the positioning of fascial entry can be tangential to the pores and skin incision web site. This is as a outcome of the stomach is insufflated with carbon dioxide at the time of trocar placement, leading to totally different fascial entry point than when the stomach is desufflated. Treatment and Prognosis Incisional hernias are best repaired with prosthetic mesh; the recurrence price is substantially decrease than after traditional tissue repair. In common, every attempt must be made to convey the fascia along with an underlay of mesh underneath the fascia to reinforce the restore. In reality, the term "stomach wall reconstruction" has been coined as a greater description for this sort of surgical procedure. This time period emphasizes the try to restore anatomy, with medialization of the parts of the abdominal wall. Every attempt is made to place a layer of peritoneum or hernia sac between the belly contents and the mesh. If diaphragmatic dysfunction (eventration disease) is suspected, the stomach wall might need to be stretched by repeated progressive pneumoperitoneum earlier than repair. There is a few suggestion that minimally invasive repair ends in fewer recurrences and decrease morbidity. Double-sided mesh is then positioned within the retroperitoneal place and glued by tacks and sutures. This strategy successfully bridges the gap rather than medializing the hernia edges.
Treatment tips for gastrointestinal stromal tumors in kids and young adults anxiety headaches buy generic effexor xr 75mg on line. Tumors that secrete hormones leading to a clinical syndrome are also identified as "useful tumors" (Table 34 anxiety network discount effexor xr online master card. The term carcinoid (karzinoide) was coined by Oberndorfer to describe a tumor that was less aggressive than an adenocarcinoma anxiety 9 year old boy effexor xr 150 mg lowest price. Mitotic figures are characteris tically infrequent (<2 mitoses/high energy field) anxiety 1894 by edvard munch discount generic effexor xr uk, and necrosis is uncommon anxiety symptoms jaw clenching purchase cheap effexor xr on line. Grade refers to the proliferative exercise of the tumor anxiety rash purchase 37.5 mg effexor xr fast delivery, measured utilizing both mitotic fee and Ki67 index. Differentiation refers to the extent to which tumor morphology resembles endocrine cells of origin. Poorly differentiated tumors are sometimes characterized as sheets of pleomorphic cells with areas of necrosis. The measurement is typical for main small intestinal carcinoids, and the tumor is subepithelial in location. B, Histopathology of a small intestinal carcinoid with its attribute insular development sample. Validations of both staging methods have been performed on inhabitants and institutional databases. Additional mutations can accumulate over time and are related to medical progression. Among functional tumors, gastrinomas are commonest (typically occurring in the duodenum). Pathophysiology and Pathology Insulinomas are nearly at all times positioned within the pancreas. Insulin is synthesized as preproinsulin by beta cells of the pancreatic islets in the rough endoplasmic reticulum. Proin sulin is liberated from preproinsulin and transferred to the Golgi apparatus. Within these granules, a protease excises the Cpeptide, and the Cpeptide and the doublestranded insulin molecule are secreted in equimolar amounts. Inherited pancreatic endocrine tumor syndromes: advances in molecular pathogenesis, analysis, administration, and controversies. Multiple endocrine neoplasia sort 1 and Zollinger-Ellison syndrome: a prospective research of 107 instances and comparability with 1009 cases from the literature. Clinical Features Insulinomas often occur in patients between 20 and seventy five years of age; 60% are girls. Hypoglycemia with fasting or train differs temporally from hypoglycemia that happens after meals (postprandial hypoglycemia), which can be brought on by many unrelated circumstances. Other less frequent causes of fasting hypoglycemia with hyperinsulinism from islet cell illness, in addition to insulinoma, include insulinomatosis, islet hyperplasia,92 and nesidioblas tosis. Most signs of insulinomas12,28,31,39,eighty two are caused by neu roglycopenia, because glucose is the primary supply of vitality for the brain. Symptoms of hypoglycemia can also be caused by cat echolamine release (adrenergic symptoms). Patients incessantly be taught to keep away from symptoms by consuming incessantly, and obesity may outcome. However, if a fasting blood glucose willpower is combined with a concomitant fasting plasma insulin level, this insulin level might be inappropriately elevated in 65% of patients with insulinoma. Seventyfive to 80% of sufferers with an insulinoma could have symptoms and a blood sugar beneath forty mg/dL inside 24 hours of starting the quick, and nearly 100% within 72 hours. In one examine,eighty five probably the most sensitive and particular standards for diagnosing insulinoma throughout a 72hour quick was the combination of a fasting glucose degree under 45 mg/dL plus an elevated proinsulin level. Invasive imaging research utilizing hepatic venous sampling after arterial calcium stimulation are hardly ever essential to localize an occult insulinoma. During a hypoglycemic episode, however, rapidly absorbable carbohydrates corresponding to fruit juices with glucose or sucrose are preferable. Diazoxide ought to be initiated at an oral dose of three to 8 mg/kg/day, divided into 2 or 3 doses per day; if not effective, diazoxide may be increased to a maximum daily dose of 15 mg/kg. Adverse results are dose associated and may restrict the power to attain maximal doses. Addition of a thiazide diuretic can correct the edema as properly as augment the hyperglycemic impact of diazoxide. Other cytotoxic systemic and liver directed therapies (discussed later) can even management hypoglycemia in sufferers with metastatic insulinomas. Treatment Treatment of insulinoma consists of controlling symptoms of hypoglycemia, adopted by tumor localization and resection. More slowly absorbed forms of carbohydrates (starches, bread, potatoes, rice) are preferable. Based on lymph node or hepatic metas tases, gastrinomas are malignant in 60% to 90% of patients. Even amongst sufferers with gastrinomas which have metastasized to the liver, the tumor progress fee is highly variable. Prospective examine of fasting serum gastrin in 309 patients from the National Institutes of Health and comparison with 2229 cases from the literature. Prospective research of gastrin provocative testing in 293 sufferers from the National Institutes of Health and comparison with 537 instances from the literature. Advances in analysis and administration of gastrinoma in patients with Zollinger-Ellison syndrome. Neurofibromatosis Type 1 and pancreatic islet cell tumours: an association which ought to be recognized. Furthermore, the low pH inactivates pancreatic lipase and can precipitate bile acids. Signs such as outstanding gastric folds on endoscopy (see left upper panel) or an imaging study. Very few patients had regular values; 60% had less than 10-fold serum gastrin will increase. Right, upper part exhibits the proportion of eighty three sufferers with primary pancreatic or duodenal gastrinomas who developed lymph node or liver metastases. Lower part exhibits proportion of 118 sufferers with major gastrinoma of varying diameter who developed lymph node or liver metastases. Prospective study of the clinical course, prognostic factors, causes of dying, and survival in patients with long-standing Zollinger-Ellison syndrome. Determinants of metastatic rate and survival in patients with Zollinger-Ellison syndrome: a prospective long-term study. The lesions are usually localized to the buttocks, groin, perineum, elbows, palms, toes, and perioral area. Sufficient antisecretory drug must be given to cut back acid hypersecretion, measured during the hour prior to the next dose of drug, to less than 10 mEq/hr in patients with out prior gastric acidreducing surgery or to less than 5 mEq/hr in patients with prior gastric acid�reducing surgical procedure. This diploma of acid suppression allows peptic lesions to heal and prevents their recurrence. Performing a duodenotomy routinely at surgery identifies more tumors than other com monly used methods. Prolonged hyperglucagonemia brought on by glucagon administration does trigger a typical rash. The similarity of the pores and skin lesions to those seen in zinc deficiencies has resulted in tri als of zinc, with some responses. Hyperglucagonemia may contrib ute to the anemia as a end result of treatment with glucagon decreases erythropoiesis in animals. The role of glucagon in causing venous thromboembolism and psychiatric issues is unsure. This dysfunction, Mahvash disease, could be reproduced in mice deficient for the glucagon receptor. Glucagonoma and the glucagonoma syndrome-cumulative expertise with an elusive endocrine tumour. Endocrine pancreatic tumors with glucagon hypersecretion: a retrospective examine of 23 instances throughout 20 years. The top of the bullae incessantly detaches or ruptures, leaving eroded areas that crust. The lesions are likely to heal within the heart whereas the sides proceed to unfold, with a crusting welldefined edge. Fusiform keratinocytes with pyknotic nuclei are often seen, as are mononuclear inflammatory infiltrates. Weight loss, typically profound and associated with anorexia, occurs in most patients,eleven,ninety,183186 even with small, nonmetastatic tumors. Mild anemia, usually normocytic and normochromic with regular serum iron, folate, and vitamin B12 ranges, can respond to profitable tumor remedy. Most glucagonoma patients have a markedly elevated plasma glucagon stage at presentation,11,12,90,182,183,186,206 with a mean plasma glucagon focus of 2110 pg/mL (range, 550 to 6600 pg/mL). Treatment Medical Treatment Initial medical therapy is directed at relieving symptoms, restoring nutritional standing, and controlling hyperglycemia as tumor localization research (discussed later) are being performed. The catabolic results of glucagon combined with glucose intolerance and diabetes mellitus can markedly have an result on the nutritional standing of those patients. Their heightened risk of venous thromboembo lism will increase postoperative morbidity. Plasma glu cagon levels lower in 80% to 90% of treated sufferers, but into the conventional range in solely 10% to 20%. Surgical Treatment Surgical resection must be considered in all sufferers with native ized tumors. The syndrome is characterised by extreme watery diarrhea, hypochlorhydria, achlorhydria, and hypokale mia (see Tables 34. The patients may require 5 or more L/day of fluid11 and over 350 mEq/day of potassium. Surgical Treatment Once the fluid and electrolyte deficits are corrected, patients should bear imaging research (discussed later) to assess tumor resectability. After performing these imaging studies, surgical treatment ought to be thought of for all patients with out metastatic dis ease. In addition to antitumor treatment, bisphosphonates can be used to management the hypercalcemia. Due to the relatively refined scientific manifestations of the somatostatinoma syndrome, this diagnosis is exceedingly rare. The median time from initial symptoms to diag nosis varies from 6 months to almost three years. Presenting symptoms/signs from the tumor embody belly ache, jaundice, and weight loss. Gastric carcinoids and neuroendocrine carcinomas: pathogenesis, pathology, and habits. For correct classification of gastric carcinoids into these varieties, the mucosa of the gastric antrum and the body/fundus ought to both be sampled, in addition to the elimination or biopsy of the lesions. Metastases are additionally more widespread in sort 2 than sort 1,116,250,257,260 and the 5year survival in sufferers with sort 2 gastric carcinoids is decrease than in type 1 (see Table 34. Neuroendocrine tumors of the stomach [gastric carcinoids] are on the rise: small tumors, small problems The 5year survival price is close to 50%, and 25% to 30% of type three patients have a tumorrelated demise. In one study253 of patients with kind 1 gastric carcinoids treated endoscopically, survival was 100% during the 46month followup; no metas tases occurred, a single affected person developed a much less differentiated tumor requiring surgery, and 64% had a recurrence after a median of eight months, handled endoscopically. For example, about 46% of tumors smaller than 1 cm are associated with liver metastases. Typical carcinoid flush involving the face and neck in a patient with small intestinal carcinoid and the carcinoid syndrome. Their tumors are related clinically to spo radic instances and share frequent aberrations in chromosome 18. They are predominantly welldifferentiated (G1) tumors, with 9% to 19% of them G2 and 2% G3. Recurrent cases of bowel obstruction may also occur, both as a result of main intestinal tumor or mesen teric metastases. Weight loss and hepatomegaly are different signs/ signs associated with these tumors. Symptoms of carcinoid coronary heart illness (dyspnea, edema) are sometimes late manifestations of illness. A separate sort of appendiceal malignancy, adenocarcinoid (also often known as goblet cell carcinoid) is completely distinct in clinical behavior and therapy. Other negative prognostic elements include location of the tumor on the base of the appendix, greater than 3 mm invasion into the mesoappendix, highgrade tumors, and positive resection margins. Standard polypectomy can often be carried out, but when local mucosal/submucosal invasion is present, a extra intensive endo scopic process may be appropriate. Pathophysiology the carcinoid syndrome occurs when sufficient concentrations of hormonal merchandise released by the tumor reach the systemic circulation. Its occurrence and severity are related to the tumor dimension in areas that drain into the systemic circulation. In greater than 90% of circumstances, this syndrome occurs with metastatic illness, espe cially to the liver. Surg Gynecol Obstet 1973;137:637�44; Norheim I, Oberg K, Theodorsson-Norheim E, et al. An analysis of 103 patients with regard to tumor localization, hormone production, and survival. J Exp Clin Cancer Res 1999;18:134�41; Norheim I, Oberg K, TheodorssonNorheim E, et al.
In broad terms anxiety symptoms lightheadedness buy generic effexor xr 150mg, the immune system can be considered a extremely structured and tightly regulated interplay between lymphoid and nonlymphoid tissues aimed at defending the host from dangerous brokers (see Chapter 2) anxiety 4 year old effexor xr 37.5mg without prescription. These extra specific B cells then depart the germinal heart anxiety 7 minute test purchase discount effexor xr on-line, enter the circulation anxiety journal 75mg effexor xr with visa, differentiate into memory B cells or antibody-producing plasma cells anxiety books buy effexor xr toronto, and return to the intestinal mucosa anxiety 30 minute therapy effexor xr 150mg sale. Some marginal zone B cells occupy the epithelial tissue that covers the Peyer patches; these cells are known as intraepithelial marginal zone B cells. The exact histogenesis of enormous B cell lymphomas doubtless varies from case to case. This article discusses the primary clinicopathologic entities that a clinician may encounter. Note the infiltration and enlargement of the mucosa by the neoplastic cells, with atrophy of the native epithelial constructions. Therefore, an evaluation of a biopsy sample by an skilled hematopathologist is extraordinarily essential to render an accurate prognosis. Thus, many remedy recommendations are primarily based on small case sequence and extrapolation from results with nodal lymphomas. Prior to the initiation of therapy with systemic chemotherapy, fascinated patients ought to receive counseling relating to fertility preservation in addition to the aspect effect profile of drugs getting used. We consider this essential as a end result of a sizeable proportion of low-grade lymphomas will bear spontaneous regression after the chronic infection driving them is satisfactorily handled. The malignant course of appears to be pushed to a large diploma by continual Hp an infection as a outcome of eradication of this an infection leads to regression of the lymphoma in 50% to 80% of circumstances. Lymphomas have also been reported in sufferers with Helicobacter heilmannii infections, with resolution after eradication of the an infection. As famous beforehand, the B cell immunoglobulin variable region (V) genes undergo somatic hypermutation through the T cell� dependent B cell response to antigen,four which leads to the manufacturing of new antigen receptors with altered antigen-binding affinity. Resultant B cell clones that categorical larger affinity antigen receptors have a survival advantage over B cell clones containing receptors with lower affinity. There are four major chromosomal translocations in extranodal marginal zone lymphomas: t(11;18)(q21;q21), t(14;18)(q32;q21), t(1;14)(p22;q32), and t(3;14)(p14. Thus, the incidence in northeastern Italy, the place the rate of Hp infection may be very high, is roughly thirteen times the incidence within the United Kingdom. It is more commonly found in advanced-stage cases, which are less prone to reply to Hp eradication. The pivotal function of Hp�reactive T cells in driving B cell proliferation could explain why tumor cells tend to remain localized and why the tumor regresses after eradication of Hp. However, continued B cell proliferation finally results in accumulation of further genetic abnormalities, resulting in autonomous progress and more aggressive clinical behavior. Because only a small proportion of Hp�infected individuals develops lymphoma, extra presently unknown environmental, microbial, or genetic elements should play a contributory position. It should be noted, however, that these lesions can generally be seen in circumstances of florid continual gastritis. Tumor cells are small to medium-sized lymphocytes, with irregularly formed nuclei and moderately plentiful cytoplasm. The morphology of those cells can vary from small lymphoplasmacytoid cells to monocytoid cells which have abundant pale cytoplasm and welldefined borders. The lymphoma cells infiltrate the lamina propria diffusely and grow around reactive follicles; the germinal facilities could also be invaded, a phenomenon termed follicular colonization. Various parameters may assist within the distinction, such as the prominence of lymphoepithelial lesions, diploma of cytologic atypia, and presence of plasma cells with Dutcher bodies (periodic acid�Schiff �positive intranuclear pseudoinclusions). Unifocal illness usually presents as ulcerated, protruding, or infiltrating plenty, however may also manifest as erosions or just erythema. Cytokeratin stain demonstrates invasion and destruction of some gastric glands by a monomorphic inhabitants of lymphocytes. Note for comparison the uninvolved regular glands in the bottom heart of the photograph. It should be famous that B cell monoclonality may be detected in Hp�associated gastritis (see Chapter 52). Additional options related to a worse prognosis are deep infiltration of the stomach wall, which is associated with a better probability of regional lymph node involvement,57 and a high percentage of large cells on histologic evaluation. Other much less widespread symptoms include anorexia, weight reduction, nausea and/or vomiting, and early satiety. The most typical web site of involvement within the stomach is the antrum, however biopsies ought to be taken from all irregular areas and randomly from each area of the stomach, as properly as the duodenum and gastroesophageal junction, as a outcome of illness is commonly multifocal. Because some lymphomas infiltrate the submucosa without involving the mucosal membrane, biopsies have to be sufficiently deep and large for histopathologic and immunohistochemical analyses. Hp an infection must be established by histologic research, breath check, or fecal antigen testing (see Chapter 52). However, it is very important recognize that the present literature on this field is less than optimum in several respects. Older studies are limited by insufficient staging procedures and outdated classification techniques. Also, none of the reports is a controlled or randomized trial, and long follow-up is lacking. Stage I Disease Most patients fall into this category and can be treated with antibiotic remedy aimed toward eradication of Hp. Follow-up endoscopy with a quantity of biopsies should be done 3 to 6 months after the completion of therapy to doc clearance of infection and to assess lymphoma regression. Patients with persistence of infection ought to be handled with a second-line antibiotic routine (see Chapter 52). The Wotherspoon index was initially proposed (1993) as a histologic device to evaluate remedy response, however its utility has been extra for initial diagnosis. Patients are then followed with endoscopy approximately every 6 months for two years and then yearly. Overall, approximately 75% of patients with stage I illness confined to the mucosa and submucosa obtain complete remission. Approximately 90% of sufferers who had a whole scientific remission to Hp eradication remain in remission,30 but late relapses can occur. Relapse may occur in affiliation with Hp reinfection and can be cured by eradicating the organism once more. Radiation or chemotherapy might be a greater choice than surgical procedure (see text) Chemotherapy for symptomatic disease. Local management with radiation or surgery could also be indicated in chosen circumstances *According to Lugano staging system. Patients with Hp infection must be handled with antibiotics to clear the infection, no matter stage (see Chapter 52). Patients with a excessive share of large cells and illness limited to the mucosa might respond to antibiotics alone, although additional study of this concern is important. Patients with a high share of large cells and more advanced-stage disease should be handled as in Table 32. The administration of patients with localized illness but a big proportion of large cells can be unsure. More latest research have documented remission after Hp eradication, in distinction to earlier research. For example, in a single research of 34 patients with high-grade histology, 18 had illness regression with Hp eradication and have been free of lymphoma after a median follow-up of seven. However, anti-Hp therapy should still be tried because of possible false-negative results for Hp or in the event that one other helicobacter, H. There is at present no consensus relating to the optimal management of this group of patients. Thus, it has become the popular therapy for patients with advancedstage disease, those who are unfavorable for Hp, and people with persistent illness despite Hp remedy. Older information means that singleagent oral chemotherapy medication such as cyclophosphamide23 or chlorambucil have exercise, as does therapy with purine analogs such as cladribine (2 CdA), which can be more practical in sufferers with t(11;18)(q21;q21). The incidence may be greater in developing than in developed nations, but clinical options appear to be related. One examine has advised that Hp infection is extra frequent in patients whose massive cell lesions had a lowgrade element. However, at this level, a precise grading system for this case has not been devised and remains a aim of ongoing analysis. Clinical Features Patients present with epigastric ache (70%) or dyspepsia (30%), signs just like those sufferers with gastric adenocarcinoma. Tumors with a low-grade element are extra likely to be multifocal than tumors with no low-grade part. Large cell lymphomas sometimes invade the muscularis propria layer or much more deeply. There is a dense infiltrate of medium-sized to massive Blymphoid cells within gastric mucosa. Approximately 70% of patients with stage I illness are disease-free 5 years after surgical procedure. In addition, the chance of gastric bleeding or perforation throughout chemotherapy is decrease than 5% and only a few of those who bleed require pressing gastrectomy. Retrospective research have shown related outcomes in sufferers treated with surgical procedure alone versus chemotherapy alone. Whether the remedy included surgical procedure was left to the discretion of every taking part center. Thus, commonplace administration of gastric large B cell lymphoma follows normal administration of nodal large B cell lymphomas. This routine is primarily based on retrospective knowledge, which exhibits increasing numbers of full remissions achieved with this routine and sufferers attaining complete remission having the most effective probability of long-term disease-free survival. Although sturdy remissions are being seen with this remedy, long-term knowledge on treatment outcomes is being discerned. However, the creating consensus seems to favor mixed chemotherapy and radiation and avoidance of surgical procedure (see text). Uncommon Gastric Lymphomas B cell lymphomas aside from marginal zone or diffuse large B cell may involve the abdomen uncommonly. T cell lymphomas of the small intestine are usually enteropathy-type intestinal T cell lymphomas; other types of T cell lymphoma have been not often reported. Patients may present with belly pain, weight reduction, obstruction, belly mass, bleeding, and/or perforation. Approximately half of sufferers have localized disease, and half have disease unfold to regional or distant nodes. Prognosis is dependent upon illness stage and affected person factors, such as age and efficiency status. Patients sometimes present with widespread adenopathy and regularly have bone marrow and extranodal involvement. The disease normally presents as a single annular or exophytic tumor,124 which can be current anyplace within the small gut; disease is usually confined to the gut or to local nodes. Some patients have acquired chemotherapy, but few data can be found relating to regimens and consequence. It must be famous that in nodal marginal zone lymphoma, chemotherapy is usually reserved for patients with signs, because the disease is slow-growing and delicate to chemotherapy, however not curable by it. As in gastric marginal zone B cell lymphoma, the small intestinal selection could have various parts of large cell transformation. Additional synchronous and metachronous lesions were present or later developed within the ileum and the duodenum, as nicely as the rectum and sigmoid colon. B, Low-power photomicrograph of ileum exhibits multiple discrete sites of mucosal and submucosal involvement by lymphomatous polyposis. Neoplastic lymphoid follicles are evident, involving the wall of the small gut and effacing the normal architecture (Hematoxylin and eosin, low power). The illness is characterised by t(14;18)(q24;q32), a translocation that leads to overexpression of the bcl-2 gene. Chemotherapy and radiation are sometimes indicated for the administration of this indolent however incurable dysfunction. Due to the superb prognosis (median survival >12 years) related to this dysfunction, most experts advocate a "wait and watch" strategy to management. The involved lymphoid tissue microscopically has a starry sky appearance caused by numerous benign macrophages that have ingested apoptotic tumor cells. Most circumstances have a translocation of the c-myc gene on chromosome eight, both to the immunoglobulin heavy-chain region on chromosome 14 or to one of the immunoglobulin light-chain regions on chromosomes 2 or 22, leading to a t(8;14), t(2;8), or t(8;22) translocation. The disease is characterized by t(11;14)(q13;q32), a translocation that leads to rearrangement and overexpression of the bcl-1 gene encoding the protooncogene cyclin D1. As famous, patients with this analysis can also current with the gross appearance of a quantity of lymphomatous polyposis. A analysis in North America or Europe ought to be questioned, except the affected person has previously lived in an endemic area. The disease occurs in people with lower socioeconomic status who reside in situations of poor hygiene and sanitation. This lack of antigen dependence is related to the event of more aggressive clinical options. Pathology Gross lesions are usually confined to the proximal small intestine, with adenopathy of adjacent mesenteric nodes. Although grossly only the proximal bowel wall is concerned, histologically the illness is characterized by a dense mucosal and submucosal cellular infiltrate that extends continuously all through the length of the small intestine. However, as already noted, numerous studies assessing immunoglobulin gene rearrangements or gentle chain restriction have instructed that even the earliest infiltrate is monoclonal. This early infiltrate broadens villi and shortens and separates crypts, however epithelial cells stay intact. This variant features a diffuse involvement of the mucosa, with lymphoid follicle-like constructions. As the illness progresses to intermediate and late stages, the villi are additional broadened and should turn out to be fully effaced, crypts are fewer, and the immunoproliferation extends extra deeply. Atypical lymphoid cells infiltrate the benign-appearing plasma cells and lymphoplasmacytic cells.
Acanthosis nigricans might suggest underlying malignancy anxiety fatigue order effexor xr 75 mg line, particularly gastric most cancers anxiety jokes buy discount effexor xr. Hematemesis is defined as vomiting of blood anxiety symptoms on one side of body buy effexor xr line, which is indicative of bleeding from the nasopharynx venom separation anxiety purchase cheap effexor xr online, esophagus anxiety symptoms or ms cheap effexor xr 150 mg without a prescription, stomach severe anxiety symptoms 247 discount effexor xr 150mg mastercard, or duodenum. Some steps may happen simultaneously or in varying order and in the emergency division, relying on the clinical scenario. Laboratory-determined hematocrit and hemoglobin values (not fingerstick hematocrit values, which are much less reliable) must be obtained each 4 to 8 hours until the hematocrit and hemoglobin values are secure. Endotracheal intubation must be thought of in sufferers with energetic ongoing hematemesis or with altered psychological status to forestall aspiration pneumonia. Emergency endoscopy before or after this interval is associated with higher mortality charges. At least 1 large-bore (14- or 16-gauge) catheter should be positioned intravenously, and a pair of ought to be positioned when the affected person has ongoing bleeding. Ideally, the affected person must be hemodynamically stable, with a coronary heart price of less than 100/min and a systolic blood strain greater than one hundred mm Hg. Middle-of-the-night endoscopy should be prevented, aside from probably the most severely bleeding or high-risk sufferers, as a result of well-trained endoscopy nurses, optimal endoscopic tools, and angiographic backup is most likely not out there at night time. In the rare patient with large bleeding and refractory hypotension, endoscopy may be performed in the working room, with the instant availability of surgical administration, if needed. Additionally, a water pump is useful for irrigating goal lesions through an adjunct channel and for diluting blood to allow suctioning, thereby facilitating visualization. A clear plastic cap placed on the tip of the endoscope may help to visualize bleeding sites behind mucosal folds, deploy endoscopic clips by modifying the angle of endoscopic approach (see later), avoid mucosal "white-out" at corners, and remove blood clots. Metoclopramide, 10 mg given intravenously before the purge and repeated each four to 6 hours, may facilitate gastric emptying and cut back nausea. In sufferers with severe or ongoing lively hematochezia, urgent colonoscopy should be carried out within 12 to 14 hours, but only after thorough cleaning of the colon. Patients with delicate or average self-limited hematochezia ought to undergo colonoscopy within 24 hours of admission after a colonic purge. A follow-up endoscopic procedure, such as single- or double-balloon enteroscopy or retrograde ileoscopy, could additionally be indicated for definitive prognosis and therapy if a focal bleeding site is found on capsule endoscopy. Complications associated to emergency endoscopy and endoscopic hemostasis could happen in as a lot as 1% of patients, depending on the type of endoscopy and remedy carried out. Deep enteroscopy* Retrograde ileoscopy (via deep enteroscopy* or colonoscopy) Source identified: Treat or laparotomy and intraoperative enteroscopy No source identified: Supportive care Endoscopic Hemostasis Thermal contact probes have been the mainstay of endoscopic hemostasis since the Nineteen Seventies. These probes are available diameters of 7 and 10 Fr and in lengths that can fit by way of panendoscopes, enteroscopes, or colonoscopes. Contact probes can physically tamponade a blood vessel to cease bleeding and interrupt underlying blood circulate; thermal vitality is then applied to seal the underlying vessel (coaptive coagulation). In animal studies, optimal coagulation has been proven to happen with low-power settings (12 to 16 W) utilized for a reasonable amount of time (8 to 10 seconds) with reasonable strain on the bleeding website. Thermal probes also can cause a coagulation injury that may make lesions bigger and deeper and may induce delayed bleeding in patients with a coagulopathy. Injection remedy is most commonly performed with a sclerotherapy needle and submucosal injection of epinephrine, diluted to a focus of 1:10,000 or 1:20,000, into or around the bleeding site or stigma of hemorrhage (see later). The advantages of this method are its broad availability, relatively low value, and safety in sufferers with a coagulopathy, and decrease risk of perforation (and absence of thermal burn damage) than thermal methods. Endoscopic hemoclips (or clips) have been out there since 1974, and have become in style following technical enhancements. Hemoclips are particularly useful for patients with malnutrition or coagulopathy39 however can additionally be difficult to deploy depending on the situation of the bleeding website, the degree of fibrosis of the underlying lesion, and limitations to endoscopic entry. Newer, large, over-the-endoscope hemoclips grasp extra tissue, adhere to fibrotic ulcers better, and might control severe ulcer bleeding higher than commonplace ulcer hemostatic methods. This method is broadly used for the therapy of esophageal varices (see Chapter 92) and can often be used for different bleeding lesions. It is relatively simple to perform, but enough mucosa have to be suctioned into the cap for ligation to be successful. Depending on the producer, some band ligation devices can solely match on diagnostic endoscopes, and switching from a bigger therapeutic endoscope to a smaller diagnostic endoscope is important. Angiography is usually diagnostic of extravasation into the intestinal lumen solely when the arterial bleeding price is a minimal of zero. The price of main problems, including hematoma formation, femoral artery thrombosis, distinction dye reactions, acute kidney injury, intestinal ischemia, and transient ischemic attacks, is 3%. Radionuclide imaging can be carried out comparatively rapidly and may help localize the general space of bleeding and thereby information subsequent endoscopy, angiography, or surgery. Caution is recommended in utilizing the results of delayed scans to localize and target lesions for surgical resection. The optimistic predictive worth, adverse predictive worth, and overall accuracy of a so-called Meckel scan have been reported to be greater than 90% in younger sufferers. The Rockall Score after endoscopic remedy correlates properly with mortality but not as properly with the chance of rebleeding. Examining all of the nonbloody mucosa rapidly is usually greatest to doc that these areas are free of any lesions. Other options to remove blood and clots are to use an endoscope with a really giant (6 mm) suction channel or to use an accessory on a therapeutic endoscope that suctions immediately via the suction port, bypassing the umbilical twine of the instrument. Raising the head of the bed also can assist transfer a clot distally from the gastric fundus. Any visualized adherent fresh blood or clot must be followed to discover its origin. If too much blood is current within the abdomen to allow detection of a bleeding lesion, another dose (or an preliminary dose) of a prokinetic agent. If bleeding from the duodenum is suspected but not recognized with a forward-viewing endoscope, a side-viewing duodenoscope ought to be used to look at the duodenal wall and ampulla. Target jet water irrigation with a foot pump through a separate small channel ought to be available. Selection of patients for early discharge or outpatient care after acute higher gastrointestinal haemorrhage. The danger of rebleeding from a peptic ulcer decreases significantly seventy two hours after the initial episode of bleeding. The prevalence of Hp infection is more than 80% of the inhabitants in lots of growing countries and 20% to 50% in industrialized nations. D, Slight oozing of blood after washing in the heart of the ulcer, with out clot or a visual vessel. B, Prior to and after endoscopic remedy, detection of arterial blood flow beneath stigmata of hemorrhage by the Doppler endoscopic probe and the mapping direction of the blood flow in the artery facilitate risk stratification, endoscopic hemostasis, and discount within the rate of rebleeding (if arterial blood circulate is obliterated). Therapy with epinephrine alone seems to be simpler when utilized in high doses (13 to 20 mL) than in low doses (5 to 10 mL). The threat is dependent upon whether or not arterial blood circulate is detected before endoscopic hemostasis (Refs. Epinephrine (1:20,000) injected in 1-mL aliquots into each of 4 quadrants should be injected around clot initially, adopted by piecemeal snare resection of the clot and therapy of underlying stigmata. Colonic diverticulum with active bleeding may be treated with epinephrine (1:20,000) injected into the neck or base. If a visual vessel is seen at the neck, it can be handled with multipolar electrocoagulation. Pressure is the tamponade stress exerted en face or tangentially through the contact probe instantly on the lesion. Power, stress, and period settings have to be reduced for small, acute, or deep bleeding lesions. The rebleeding rate for ulcers with an adherent clot handled with medical remedy alone is 8% to 35%, with most giant research reporting rebleeding rates of 30% to 35%. Clean-Based Ulcers Patients with a clean-based ulcer at endoscopy after target irrigation have a rebleeding fee of lower than 5%. When combination therapy is carried out, coagulation is carried out with a large 10 Fr multipolar probe. The probe is then removed slowly from the ulcer (sometimes with light irrigation to stop pulling coagulated tissue), and thermal coagulation is repeated as required to stop bleeding and flatten any underlying seen vessel. With profitable endoscopic hemostasis, the rebleeding rate may be decreased to 30% with monotherapy and 15% with combination therapy (see Table 20. Alternatively, injection of epinephrine followed by hemoclip placement instantly across the actively bleeding website can be effective. Some investigators recommend that clips be positioned prior to injection of epinephrine to allow placement of the clip immediately on the vessel somewhat than on a submucosal epinephrine-filled cushion. B, After injection of epinephrine, oozing has subsided; the edge of the ulcer is seen inferior to clot. The combination technique decreases the rebleeding rate from up to 35% (with medical therapy alone) to 5%. Monotherapy with a thermal probe or epinephrine injection reduces the rebleeding fee to lower than 5%. In patients with oozing, the bleeding arteries could additionally be small and the outcomes are better than these in sufferers with lively arterial bleeding. B, the nonbleeding seen vessel is injected with epinephrine, after which blanching and swelling of surrounding mucosa occur. D, After completion of treatment, the visible vessel has been coagulated and flattened. B, the clot was injected with epinephrine, followed by piecemeal snare polypectomy to trim away the clot (C-E), after which an underlying vessel was revealed (F [arrow]). If the affected person has a clean-based gastric ulcer, biopsies of the ulcer edge and gastric muscosa ought to be considered to exclude underlying malignancy (see Chapter 53). Therefore the danger of rebleeding is excessive, and definitive hemostasis with standard techniques is often required in sufferers with varices or ulcers with main stigmata. Current tips suggest utilization of hemospray as a stopgap or adjunct approach. Testing for Hp Infection In a affected person with a bleeding gastric or duodenal ulcer, endoscopic mucosal biopsy specimens of the normal-appearing antrum and mid-body higher curvature should be obtained to assess for the presence of Hp infection. Biopsy specimens can be obtained safely after successful endoscopic hemostasis, but bleeding reduces the sensitivity of speedy urease testing. Therefore stool antigen and other exams for Hp infection are really helpful (see Chapter 52). The rebleeding rate in the omeprazole-treated group was 11% in contrast with 36% in the placebo-treated group (P < zero. Second-Look Endoscopy Routine repeat, or second-look, endoscopy 24 hours after initial endoscopic hemostasis, with additional endoscopic hemostasis if persistent high-risk endoscopic stigmata are found, has been proposed as a method to improve affected person outcomes. Rebleeding After Endoscopic Treatment the danger of rebleeding from peptic ulcers, which started bleeding within the outpatient setting and required endoscopic hemostasis, is best within the first seventy two hours after analysis and therapy. The difference between ulcer hemorrhage that starts within the outpatient setting and hemorrhage that starts within the inpatient setting is substantial (Table 20. Further research are warranted in this high-risk group to define optimal administration. Factors that predicted failure of endoscopic retreatment included an ulcer size of no much less than 2 cm and hypotension on initial presentation. This new therapy has the potential to cut back the necessity for surgery or angiography for recurrent ulcer bleeding. After successful endoscopic therapy and recovery from sedation, the patient can be started on a liquid food regimen, with subsequent advancement of the diet. Intermediate-Risk Stigmata Patients with flat spots and arterial blood circulate detected beneath, those with oozing bleeding from an ulcer and no other stigmata. Angiography, Surgery, and Over-the-Scope Hemoclips Patients with recurrent bleeding despite 2 classes of endoscopic hemostasis can be thought-about for angiographic embolization or surgical remedy. If the patient can also be positive for Hp, the organism ought to be eradicated with normal remedy (see Chapter 52). Endoscopy with biopsies and brushings is important for making these diagnoses and determining the suitable pharmacologic remedy (see Chapter 45). Ulcer Hemorrhage in Hospitalized Patients Hemorrhage from an ulcer or erosions in hospitalized sufferers usually falls into 2 categories. Diffuse oozing is common, and sufferers have a poor prognosis and high rebleeding fee, often related to impaired wound therapeutic and multiple organ failure. The 2 primary risk factors are severe coagulopathy and mechanical air flow for longer than 48 hours. In areas of the world where the inhabitants is at intermediate danger for gastric most cancers, 2% to 4% of repeat upper endoscopies to affirm ulcer therapeutic have been reported to disclose gastric cancer. It is normally located within the gastric fundus, within 6 cm of the gastroesophageal junction, though lesions in the duodenum, small intestine, and colon have been reported. The cause is unknown, and congenital and acquired (related to mucosal atrophy or an arteriolar aneurysm) causes are thought to happen (see Chapter 38). The tear is assumed to end result from increased intra-abdominal strain, together with a shearing impact caused by unfavorable intrathoracic pressure above the diaphragm, which is usually associated to vomiting. Mallory-Weiss tears have been reported in patients who vomit while taking a bowel purge earlier than colonoscopy. A retroflexed view within the stomach might provide higher visualization than a ahead view. Usually, the bleeding is self-limited and delicate, but sometimes it might be extreme, especially in sufferers with esophageal varices or coagulopathies. Mucosal (superficial) Mallory-Weiss tears can start therapeutic within hours and may heal fully inside forty eight hours. The administration of sufferers with esophageal varices caused by portal hypertension who even have a Mallory-Weiss tear ought to be focused toward the esophageal varices, with esophageal band ligation or variceal sclerotherapy (see later and Chapter 92). The tumors are normally massive, ulcerated masses within the esophagus, abdomen, or duodenum.
Order genuine effexor xr on-line. Anxiety Definition - What You MUST Know.