
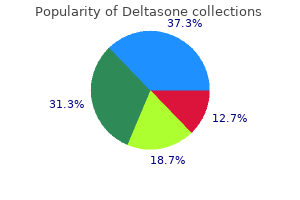
Margaret Mary Showel, M.D.
- Assistant Professor of Oncology

https://www.hopkinsmedicine.org/profiles/results/directory/profile/0021061/margaret-showel
The efficacy of these strategies is mostly comparable allergy testing houston order deltasone 5mg online, besides that epinephrine injection alone is inferior to the opposite modalities but can be helpful when combined with any of the others allergy medicine active ingredient order deltasone 40 mg line. Pre-endoscopy administration of intravenous proton pump inhibitor therapy (at a dose equivalent to a bolus of eighty mg esomeprazole allergy testing york hospital purchase 20mg deltasone mastercard, followed by a steady infusion of eight mg/hour till endoscopy) reduces bleeding and the need for emergent endoscopic treatment allergy shots for ragweed discount 20 mg deltasone visa, nevertheless it has no impact on the need for transfusion or the prevalence of rebleeding or dying allergy testing rast buy deltasone with visa. For patients with active bleeding or stigmata of recent bleeding allergy symptoms to dogs purchase genuine deltasone, endoscopic treatment must be followed by an intravenous proton pump inhibitor given as a bolus at a dose equal to eighty mg esomeprazole over 30 minutes, adopted by a steady infusion at a dose equal to esomeprazole 8 mg/hour for seventy two hours, to cut back rebleeding and the necessity for further intervention. Intermittent oral or intravenous therapy at 6- to 12-hour intervals in a cumulative daily dose equal to eighty to a hundred and sixty mg esomeprazole may be equally efficient, though more proof is needed in patients from Western nations. Unless a particular contraindication exists, emergency surgery is often indicated,10 though extra conservative approaches are typically acceptable. Given the success in attaining the long-term cure of ulcer disease through the eradication of H. Intractability is a term strictly applied to an ulcer that persists even after intensive and prolonged proton pump inhibitor remedy. These uncommon instances may end result from poor compliance with beneficial therapy, surreptitious use of ulcerogenic medication, or other diseases. If these points are recognized and these diagnoses are pursued, additional complications and interventions similar to surgical vagotomy and pyloroplasty can virtually at all times be averted. Acid peptic disease related to alcohol or bisphosphonates should be addressed by discontinuing the precipitating agent. Treatment of Zollinger-Ellison syndrome requires high-dose proton pump inhibitors and/or surgery (Chapter 219). Those rare ulcers attributable to Crohn disease (Chapter 132), vasculitis (Chapter 254), sarcoidosis (Chapter 89), polycythemia vera (Chapter 157), amyloidosis (Chapter 179), and other uncommon problems must be addressed by treating the underlying situation. Stress ulcers and Cameron ulcers are handled by potent acid suppressive therapy. About 70 to 80% of rebleeds happen within the first 3 days and generally should be managed by repeat endoscopy. If endoscopy fails to stop the bleed or forestall additional rebleeding, surgery and interventional radiology are equal options. Surgery includes stitching of the ulcer and occlusion of the feeding artery, often the gastroduodenal artery. Interventional radiology uses angiography to insert coils within the offender vessel at the website of the bleed. Single-center observational expertise suggests that each of those methods is equally efficient within the palms of experienced clinicians, and the choice is dependent upon local availability and experience. The threat for a deadly consequence of an upper gastrointestinal hemorrhage may be estimated based mostly on 5 clinical and endoscopic parameters (see Table 130-5). In several studies, mortality in sufferers with a bleeding peptic ulcer was lower than 2% among those with a rating of 2 points or much less, 10% in these with 3 to 5 points, and up to 46% in these with 6 points or extra. Management of sufferers who get well after a peptic ulcer hemorrhage is much like the therapy of patients with uncomplicated ulcers. In patients with a history of ulcer bleeding and concomitant cardiovascular disease requiring antiplatelet remedy, the mixture of low-dose aspirin and a proton pump inhibitor at a dose equivalent to esomeprazole 20 mg twice daily is associated with a decrease risk for sophisticated ulcer than is clopidogrel monotherapy. If a affected person who requires antiplatelet therapy presents with a bleeding ulcer, antiplatelet therapy must be continued or restarted as quickly as potential if the risk for a cardiovascular event outweighs the danger for recurrent bleeding. Intractability Stenosis Perforation Perforation might manifest as an acute occasion, whereby gastric contents spill into the peritoneal cavity, or extra insidiously because the ulcer slowly penetrates into surrounding tissues. Acute free perforation sometimes causes abrupt and severe abdominal pain associated with stomach muscular spasm that produces boardlike rigidity of the stomach and other manifestations of peritoneal irritation. Leukocytosis and elevated C-reactive protein ranges develop rapidly, and delicate hyperamylasemia could occur. Most sufferers who develop clinically relevant gastric outlet obstruction have had an ulcer in the duodenal bulb and/or pyloric channel. Edema and inflammation play an essential position, and sometimes a patient with active disease presents with signs of outlet obstruction as manifested by nausea, vomiting, and gastric stasis with no tight, continual stenosis. The first is nasogastric tube aspiration and gastric lavage to clear the abdomen of retained debris, followed by early endoscopy. Nasogastric suction may need to be maintained for a quantity of days if vomiting resumes when the tube is clamped. The second step consists of intense antisecretory therapy utilizing intravenous proton pump inhibitors in a dose equal to a bolus of eighty mg esomeprazole over 30 minutes, adopted by a steady infusion of eight mg/hour. The four major issues are intractability, perforation, hemorrhage, and stenosis. Patients with sophisticated ulcer illness are at specific danger for recurrent complications and wish careful assessment for secondary prevention. In patients who take long-term acid suppressive remedy, especially with proton pump inhibitors, the risks for community-acquired pneumonia and vitamin B12 deficiency (Chapters a hundred and fifty five and 205) are increased. Helicobacter pylori eradication remedy for useful dyspepsia: systematic evaluation and meta-analysis. Eradication remedy for peptic ulcer disease in Helicobacter pylori-positive individuals. Efficacy of probiotic supplementation remedy for Helicobacter pylori eradication: a meta-analysis of randomized managed trials. Concomitant, bismuth quadruple, and 14-day triple therapy in the first-line therapy of Helicobacter pylori: a multicentre, open-label, randomised trial. Systematic review and meta-analysis: susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. Sequential versus normal triple first-line therapy for Helicobacter pylori eradication. Systematic evaluate and network meta-analysis: comparative effectiveness of therapies for second-line Helicobacter pylori eradication. Proton pump inhibitors for stopping non-steroidal anti-inflammatory drug induced gastrointestinal toxicity: a systematic evaluate. Similar efficacy of proton-pump inhibitors vs H2-receptor antagonists in reducing threat of upper gastrointestinal bleeding or ulcers in high-risk users of lowdose aspirin. Efficacy and safety of stress ulcer prophylaxis in critically sick sufferers: a network meta-analysis of randomized trials. Effects of gastroprotectant medicine for the prevention and therapy of peptic ulcer disease and its problems: a meta-analysis of randomised trials. Restrictive versus liberal blood transfusion for gastrointestinal bleeding: a scientific evaluate and meta-analysis of randomised controlled trials. Epinephrine injection versus epinephrine injection and a second endoscopic methodology in high-risk bleeding ulcers. Global prevalence of Helicobacter pylori an infection: systematic evaluation and meta-analysis. Associations between cytokine gene polymorphisms and susceptibility to Helicobacter pylori infection and Helicobacter pylori related gastric most cancers, peptic ulcer disease: a meta-analysis. Antibiotic resistance of Helicobacter pylori to sixteen antibiotics in clinical patients. Management of Helicobacter pylori an infection: the Maastricht V/Florence consensus report. Helicobacter pylori an infection: an update for the internist in the age of increasing international antibiotic resistance. The risks and advantages of long-term use of proton pump inhibitors: skilled review and best apply recommendation from the American Gastroenterological Association. Cryptococcosis Answer: D In vitamin B12 deficiency with pernicious anemia, gastric atrophy is brought on by an autoimmune gastritis. Systemic mastocytosis is, nevertheless, related to a clearly increased risk for peptic ulceration. Chronic active gastritis Answer: A Patients with complicated peptic ulcer illness, similar to peptic ulcer bleeding, are at considerably increased danger for recurrent ulcer issues. Which of the next statements is false in patients with peptic ulcer bleeding Answer: E In patients with peptic ulcer bleeding, endoscopic remedy is the mainstay to cease ongoing bleeding and cut back the risk for rebleeding. The Blatchford scale can be utilized to predict the need for intervention, similar to endoscopic remedy and blood transfusion; a low rating is associated with a low probability that an intervention is needed. If this retreatment fails, each angiographic embolization of the feeding vessel and surgical procedure are alternative rescue therapies. None of the above Answer: B Zollinger-Ellison syndrome is caused by a gastrin-producing endocrine tumor, which is usually within the pancreas or small bowel and leads to marked hyperacidity. This syndrome often provides rise to extreme peptic ulcer disease with multiple, concomitant duodenal ulcers which would possibly be proof against conventional acid suppressive therapy. An 80-year-old girl with degenerative joint illness involving her fingers presents with a gastric ulcer with easy edges. Which of the next is the main factor contributing to current modifications within the incidence of peptic ulcer disease in developed international locations In the United States, norovirus has surpassed rotavirus because the leading cause of gastroenteritis requiring medical care. Approximately 48 million Americans undergo from food-borne illness each year, together with about a hundred thirty,000 annual hospitalizations and 3000 deaths, most in aged people. The major pathogens that cause diarrhea result in an estimated $14 to sixteen billion in annual well being care prices and days lost from work. As a symptom, diarrhea could be described as a decrease in stool consistency (increased fluidity), stools that cause urgency or belly discomfort, or a rise in the frequency of stool. Consistency is outlined because the ratio of fecal water to the water-holding capacity of fecal insoluble solids, which are composed of bacterial mass and dietary fiber. As a sign, diarrhea is defined by the burden or volume of stool measured over a 24- to 72-hour period. Chronic diarrheal situations persist for a minimum of 4 weeks and, more typically, 6 to eight weeks or longer. The 4 mechanisms of diarrhea are osmotic, secretory, exudative, and altered motility. Diarrhea is the second main reason for mortality worldwide and is especially problematic for elderly individuals and for children youthful than 5 years of age in creating nations. Infectious diarrheal situations cause approximately 525,000 worldwide childhood deaths annually, regardless of the improved use of oral rehydration options, zinc, and vitamin A supplements. The permeable duodenum then renders the meal roughly isotonic with an electrolyte content just like that of plasma by the time it reaches the proximal jejunum. In the colon, K+ is secreted, and the Na+ transport mechanism of the colonocyte, along with the low epithelial permeability, extracts Na+ and fluid from the stool. As a end result, the Na+ content of stool decreases to 30 to forty mmol/L; K+ increases from 5 to 10 mmol/L within the small bowel to seventy five to 90 mmol/L; and poorly absorbed divalent cations, similar to Mg2+ and Ca2+, are concentrated in stool to values of 5 to a hundred mmol/L. The anion concentrations within the colon change drastically as a end result of bacterial degradation of carbohydrate. In the setting of carbohydrate malabsorption, the generation of high concentrations of these short-chain fatty acids could decrease stool pH to 4 or lower. Stimulation of secretion by neurotransmitters, hormones, and inflammatory mediators (Table 131-1) can offset this steadiness. Diarrhea is due primarily to alterations of intestinal fluid and electrolyte transport and fewer to clean muscle function. The diet supplies 2 L of this fluid; the rest comes from salivary, gastric, hepatic, pancreatic, and intestinal secretions. Diarrhea can result from increased secretion by the small intestine or the colon if the maximal day by day absorptive capacity of the colon (4 L) is exceeded. A appreciable proportion of the osmolality of stool results from the nonabsorbed solute. This hole between stool osmolality and the sum of the electrolytes within the stool causes osmotic diarrhea. Active chloride secretion or inhibited sodium absorption, which additionally creates an osmotic gradient favorable for the motion of fluids from blood to lumen, explains the pathophysiology of the secretory diarrheas. There are many infectious, dietary/drug, gastrointestinal, extraintestinal, and surgical causes. An understanding of the physiology and pathophysiology of nutrient digestion and intestinal absorption can information the diagnostic approach. This article supplies an understanding of key concepts of intestinal physiology, pathophysiology, and clinical presentation to make a selected diagnosis in patients who present with diarrhea or suspected malabsorption. A, sodium is absorbed by nutrient-dependent and -independent transport processes in the small intestine and by a sodium channel (enac) within the colon. Glucocorticoids additionally inhibit release of arachidonic acid and production of prostaglandin by inflammatory cells. DrA (slc26) = down-regulated in adenoma gene; nhe (slc9) = sodium-hydrogen exchanger. Inflammatory diarrheas, which can be watery or bloody, are characterized by enterocyte harm, villus atrophy, and crypt hyperplasia. The broken enterocyte membrane of the small gut has decreased disaccharidase and peptide hydrolase exercise, lowered or absent Na+-coupled sugar or amino acid transport mechanisms, and reduced or absent sodium chloride absorptive transporters. If the irritation is severe, immunemediated vascular damage or ulceration allows blood, pus, and protein to leak (exudate) from capillaries and lymphatics and contribute to the diarrhea. Approximately 80% of acute diarrheas are due to infections with viruses, bacteria, and parasites. The remainder are because of medicines which have an osmotic force, stimulate intestinal fluid secretion, harm the intestinal epithelium, or contain poorly absorbable or nonabsorbable sugars. Also phenolphthalein, anthraquinone, bisacodyl, dioctyl sodium sulfosuccinate, and senna. Most infectious diarrheas are acquired via fecal-oral transmission from water, meals, or person-to-person contact (Table 131-2).
Magnesium deficiency can happen allergy testing arm discount 20 mg deltasone otc, hardly ever allergy medicine bloody nose order online deltasone, in protein-calorie malnutrition and may be associated with acute hypomagnesemia during refeeding due to rapid cellular magnesium uptake allergy testing your baby purchase deltasone pills in toronto. Fat malabsorption in circumstances such as celiac illness allergy testing austin tx discount deltasone 5 mg with amex, Crohn disease allergy testing uk reviews order genuine deltasone on-line, and small intestinal resection causes magnesium deficiency as a result of free fatty acids accumulate within the intestinal lumen allergy shots bad for you order deltasone visa, where they mix with magnesium to form insoluble soaps. Proton pump inhibitors also can cause hypomagnesemia, primarily in patients concurrently utilizing diuretics. Lower gastrointestinal tract secretions are rich in magnesium, so diarrhea of colonic origin is a standard explanation for hypomagnesemia. Sweat contains important quantities of magnesium, and transient hypomagnesemia can occur after extended, intense train such as marathon runs. Magnesium is also misplaced from burned pores and skin surfaces, and 40% of patients with severe burns (Chapter 103) are hypomagnesemic. In patients with extreme hyperparathyroidism (Chapter 232) and excessive bone turnover, continued sequestration of minerals inside bone after parathyroidectomy causes transient hypocalcemia, hypomagnesemia, and hypophosphatemia. Renal magnesium losses can occur in the restoration section of acute tubular necrosis or urinary tract obstruction. Inhibition of sodium reabsorption within the thick ascending limb of Henle by loop diuretics and within the distal convoluted tubule by thiazide diuretics inhibits tubular magnesium reabsorption and results in urinary magnesium wasting. Tubular toxins which may be common causes of renal magnesium losing embrace cisplatin, carboplatin, amphotericin B, and aminoglycosides, which are often related to hypokalemia and infrequently with renal tubule acidosis, as nicely as calcineurin inhibitors such as cyclosporine and tacrolimus, which additionally cause hyperkalemia. Antibodies to the epidermal progress factor receptor, similar to cetuximab and panitumumab, which are used to treat metastatic colorectal cancer, downregulate a distal tubule magnesium channel and cause isolated severe hypomagnesemia. The average daily consumption of magnesium is 300 mg, the principle sources of that are green greens, nuts, complete grain cereals, milk, and seafood. In the kidney, 70 to 80% of serum magnesium is filtered at the glomerulus, with the bulk being reabsorbed along the size of the tubule, particularly within the thick ascending limb of Henle. In states of magnesium deficiency or excess, renal tubule reabsorption is tightly regulated in order that magnesium excretion is adjusted accordingly. Disorders of magnesium and phosphate homeostasis-especially hypomagnesemia, hypophosphatemia, and hyperphosphatemia within the setting of kidney disease-are frequent and most often asymptomatic. This article critiques the causes of magnesium and phosphate problems, checks and algorithms to diagnose the underlying cause, and therapy options, including replacement regimens. Mild-to-moderate hypomagnesemia or magnesium deficiency is frequently asymptomatic. Manifestations of increased neuronal excitability are the commonest symptoms, together with paresthesias, tetany, and seizures. These could also be associated with Chvostek sign (twitching of the cheek muscle tissue in response to tapping the facial nerve in front of the ear) or Trousseau signal (carpal spasm induced by compressing the upper arm with a tourniquet or blood strain cuff). Coexistent hypokalemia is very common for 2 causes: lots of the causes of hypomagnesemia are also causes of potassium loss, and hypomagnesemia itself causes renal potassium wasting. Severe hypomagnesemia additionally impairs parathyroid hormone secretion and induces tissue resistance to its actions, thereby resulting in hypocalcemia. Mild hypermagnesemia (serum magnesium level > 4 to 6 mg/dL) causes hypotension, nausea, vomiting, facial flushing, urinary retention, and ileus. Above serum levels of 8 to 12 mg/dL, flaccid skeletal muscle paralysis and hyporeflexia may ensue, along with bradyarrhythmias, respiratory despair, coma, and cardiac arrest. In the occasion of great toxicity, the effects of magnesium could be temporarily antagonized by the administration of intravenous calcium salts (5 to 10 mL of 10% calcium chloride). Renal magnesium excretion may be enhanced by administering furosemide (20 to 40 mg each four hours) along with a saline infusion (0. In sufferers with superior renal insufficiency, the best method of magnesium elimination is hemodialysis. It is a significant component of bone mineral, of phospholipids in cell membranes, and of nucleic acids. Of the whole body phosphorus content material, 85% is in bone, 14% is in intracellular compartments, and solely 1% is in extracellular fluid. The kidneys excrete excess phosphorus, which is the principal mechanism by which the physique regulates extracellular phosphate stability. Ninety p.c of serum phosphate is filtered on the glomerulus, of which 80 to 97% is reabsorbed along the nephron, primarily within the proximal tubule. Parathyroid hormone will increase renal phosphate excretion by inhibiting the sodium-phosphate cotransporter within the proximal tubule, whereas vitamin D enhances intestinal phosphate absorption. In delicate circumstances or within the outpatient setting, oral magnesium salts corresponding to magnesium oxide (250 to 500 mg 4 times daily) can be utilized for repletion, however these substances frequently trigger diarrhea, significantly at high doses. In the inpatient setting, intravenous magnesium sulfate (1 to 2 g each 6 hours) can be utilized for repletion. Because the redistribution of magnesium from extracellular to intracellular compartments is relatively slow, the serum magnesium focus may normalize earlier than whole physique magnesium shops are replete. It is therefore prudent to continue intravenous magnesium for an extra 1 to 2 days after restoration of normomagnesemia. In sufferers with regular renal perform, any excess magnesium is solely excreted renally. Adverse results from intravenous magnesium administration are primarily because of transient hypermagnesemia and include flushing, hypotension, and flaccid paralysis. However, in patients with persistent magnesium losing, similar to in Gitelman syndrome (Chapter 119), it may be tough to sustain with the continuing losses with oral remedy. Fortunately, these individuals are inclined to adapt to their persistent hypomagnesemia and tolerate it fairly nicely. Transient hypermagnesemia can occur in patients given large doses of intravenous magnesium, for example, within the setting of preeclampsia. Phosphate is regularly depleted in alcoholism (Chapter 30) due to the intake of a carbohydrate-rich, phosphate-poor diet, in addition to renal phosphate losing. Divalent cation-containing antacids bind phosphate within the intestinal lumen to form insoluble salts, thereby stopping their absorption. Vitamin D deficiency also leads to decreased intestinal phosphate absorption and hence to hypophosphatemia. Respiratory however not metabolic alkalosis (Chapter 110) might cause transient hypophosphatemia. In this disorder, intracellular pH is elevated, thereby stimulating glycolysis, which depletes the intracellular inorganic phosphate pool and results in a shift of phosphate into cells. The cause of hypophosphatemia is often evident from the history and bodily examination. Similarly, in malnourished patients (Chapter 203), whose complete body phosphate stores could also be depleted, overzealous intravenous refeeding with carbohydrate-rich fluids may stimulate insulin launch and cause acute hypophosphatemia. The tyrosine kinase inhibitors imatinib, sorafenib, and nilotinib, that are used in the treatment of assorted cancers (Chapters 169 and 175), can cause profound hypophosphatemia, which appears to be due either to inhibition of bone resorption or a partial Fanconi syndrome. Renal phosphate wasting is normally as a result of impaired proximal tubule phosphate reabsorption. In primary hyperparathyroidism (Chapter 232), hypercalcemia is typically related to hypophosphatemia. Phosphaturia can also occur with diuretics, particularly carbonic anhydrase inhibitors, and with antimicrobial brokers similar to pentamidine and foscarnet. Oncogenic osteomalacia is a paraneoplastic syndrome (Chapters 169 and 231) associated primarily with mesenchymal tumors that secrete a selection of phosphaturic elements collectively often recognized as phosphatonins. A related phenotype is present in X-linked and autosomal dominant hypophosphatemic rickets; these inherited problems are characterised by a rise in a circulating phosphatonin called fibroblast growth factor-23. Phosphatonins inhibit both renal tubular phosphate reabsorption and 1-hydroxylation of 25-hydroxycholecalciferol, thereby resulting in hypophosphatemia, rickets, or osteomalacia (Chapter 231) and inappropriately low serum ranges of 1,25-dihydroxycholecalciferol. Finally, patients undergoing renal substitute therapy by steady venovenous hemodiafiltration typically become phosphate-depleted and want ongoing replacement. Manifestations of severe hypophosphatemia include encephalopathy, dilated cardiomyopathy, generalized muscle weakness that may lead to respiratory failure, rhabdomyolysis, and hemolysis. Hypophosphatemia also impairs renal ammoniagenesis and reduces the availability of urinary buffer, thereby impairing renal acid excretion and inflicting metabolic acidosis. Oral repletion can be achieved with sodium or potassium phosphate salts (1 to 2 g/day) or with skimmed milk. Hypophosphatemia in patients on continuous venovenous hemodiafiltration could be ameliorated by method of phosphate-containing dialysate and alternative options. The phosphorus in some laxatives and enemas could also be absorbed and cause hyperphosphatemia. Intoxication with vitamin D or its analogues increases intestinal absorption of each calcium and phosphorus. Patients with diabetic ketoacidosis (Chapter 216) are often hyperphosphatemic at preliminary evaluation because of the redistribution of phosphate out of cells in the insulin-deficient state. Decreased phosphate excretion is most commonly because of acute or continual renal failure (Chapter 121). With a standard food plan, serum phosphate ranges could be maintained throughout the normal vary until the glomerular filtration rate falls under 25 mL/ minute. Finally, because parathyroid hormone stimulates proximal tubule phosphate excretion, major hypoparathyroidism (Chapter 232) is commonly associated with mild hyperphosphatemia together with hypocalcemia. Acute hyperphosphatemia will increase the chance for precipitation of calcium phosphate and subsequent metastatic calcification in soft tissues, including the kidney, during which it may possibly cause acute renal failure. In the persistent hyperphosphatemia of chronic renal insufficiency, sufferers with a serum phosphate focus greater than 6. Hyperphosphatemia on this setting is a risk issue for coronary and different vascular calcification, which is related to elevated mortality. In symptomatic patients and people with impaired renal operate, phosphate ought to be removed by extracorporeal therapy. Because of the gradual price of phosphate mobilization from intracellular stores, steady venovenous hemodiafiltration is significantly simpler than intermittent hemodialysis. Chronic hyperphosphatemia (Chapter 121) could be managed by minimizing dietary phosphorus intake8 and administering oral phosphate binders such as calcium salts. Data counsel that non�calcium-based phosphate binders A1 and especially sevelamer A2 might reduce all-cause mortality compared with calcium-based binders in sufferers with chronic kidney illness. Severe acute hyperphosphatemia can be life-threatening owing to metastatic calcification and multiorgan failure, nevertheless it typically responds well to immediate remedy. Chronic hyperphosphatemia in patients with persistent kidney failure (Chapter 121) is commonly pretty resistant to treatment, particularly in poorly compliant individuals, and is associated with elevated long-term mortality. Effect of calcium-based versus non-calcium-based phosphate binders on mortality in sufferers with chronic kidney illness: an updated systematic review and meta-analysis. Magnesium and well being outcomes: an umbrella evaluation of systematic evaluations and meta-analyses of observational and intervention studies. Serum magnesium concentrations and all-cause, cardiovascular, and cancer mortality among U. Phoxilium() reduces hypophosphataemia and magnesium supplementation during continuous renal substitute remedy. Admission hyperphosphatemia increases the danger of acute kidney damage in hospitalized sufferers. Routine laboratory examination revealed the following: serum sodium 133 mEq/L, potassium 2. Answer: B this affected person has hypophosphatemia, hypokalemia, a probable hyperchloremic metabolic acidosis, hypouricemia, and glycosuria without hyperglycemia. Tenofovir can also trigger acute tubular necrosis and acute kidney injury, but these scientific syndromes would are inclined to improve the serum phosphate focus. A 34-year-old man presents with muscle soreness and voiding darkish brown urine quickly after initiating a high-intensity house train regimen. Answer: E this patient has rhabdomyolysis, as evidenced by the very high creatine kinase value. Hyperkalemia and hyperphosphatemia resulting from release of intracellular ions is typical on this disease. Given the degree of renal insufficiency and concomitant hyperkalemia, extracorporeal remedy with either hemodialysis or steady venovenous hemodiafiltration could be acceptable and would successfully take away phosphate. Forced saline or alkaline diuresis is contraindicated in the setting of renal insufficiency. Insulin would shift some phosphorus into cells, however this may not have a big or lasting effect. Sodium bicarbonate can be used in an attempt to alkalinize the urine, which is believed to decrease the renal toxicity of myoglobin, however it would not have an result on the phosphate degree. A 55-year-old lady with ovarian cancer is being treated with carboplatin, Taxol, and pelvic irradiation. She now complains of continual diarrhea and is found to have the next blood serum ranges: magnesium zero. Answer: A the fractional excretion of magnesium is 68%, thereby indicating that the cause for the hypomagnesemia is severe renal magnesium wasting somewhat than diarrheal losses. Platinum-based chemotherapeutic brokers, which are poisonous to the renal tubule, are a well-recognized reason for hypomagnesemia. This toxicity, which is more widespread with cisplatin but also has been reported with carboplatin, can persist after discontinuation of remedy. The hypocalcemia on this case is likely secondary to the extreme hypomagnesemia, which impairs parathyroid hormone secretion and also causes peripheral resistance to its actions. Answer: D Magnesium ingestion in patients with renal insufficiency may cause hypermagnesemia. Hypotension, flaccid muscle paralysis, and hyporeflexia are typical manifestations. Hypermagnesemia could be handled by antagonizing the consequences of magnesium with intravenous calcium salts, by growing the excretion of magnesium with furosemide, or by hemodialysis.
His blood check outcomes had been positive for elevated alanine aminotransferase (82 U/L; regular allergy medicine nose spray order 40mg deltasone, forty five U/L) allergy medicine makes you drowsy generic deltasone 5 mg, blood glucose (181 mg/dL; regular allergy medicine during 3rd trimester order deltasone 40mg visa, <125 mg/dL) allergy medicine purple box purchase cheap deltasone on line, and hemoglobin A1c (9%; regular allergy joint pain cheap deltasone generic, <7%) allergy forecast kyle texas cheap deltasone 5 mg on line. Glycogen storage disorder Answer: B Tender hepatomegaly, elevated alanine aminotransferase level, and echogenic liver by ultrasound evaluation are suggestive of some form of infiltrative liver disorder. Glycogen accumulation also enhances echogenicity on ultrasound examination and should mimic fatty liver. It is believed that hyperinsulinemia is needed for growth of nonalcoholic fatty liver illness. She is a heavy drinker and has been consuming more than 7 drinks of vodka every night for the previous 5 years. Physical examination reveals an emaciated woman with deep scleral icterus, peripheral muscle wasting, tender hepatomegaly, and pedal edema. Laboratory take a look at results present macrocytic anemia, gentle leukocytosis, elevated aminotransferase levels, and direct bilirubinemia. Most transplant centers require up to 6 months of total abstinence and a few type of behavioral remedy for underlying alcoholism. In eligible sufferers, 28 days of oral prednisolone improves short-term survival in people with acute alcoholic hepatitis. Similarly, some earlier medical investigations have proven promising outcomes for N-acetylcysteine and enteral diet. These "regenerative" nodules lack normal lobular organization and are surrounded by fibrous tissue. Although cirrhosis is histologically an "all-or-nothing" prognosis, it can be categorized clinically by its status as compensated or decompensated. Decompensated cirrhosis is defined by the presence of ascites, variceal bleeding, encephalopathy, or jaundice, that are problems that end result from the main penalties of cirrhosis: portal hypertension and liver insufficiency. The prevalence of continual liver illness or cirrhosis worldwide is estimated to be a hundred (range, 25 to 400) per 100,000 topics, nevertheless it varies widely by nation and by geographic area. Cirrhosis is a vital explanation for morbidity and mortality worldwide and within the United States. According to the World Health Organization, about 800,000 individuals die of cirrhosis annually. In the United States, cirrhosis accounts for about 32,000 deaths every year, or a demise rate of 10. As chronic liver illness impacts people in their best years of life, it has a significant impression on the financial system because of untimely demise, illness, and incapacity. Chronic viral hepatitis C and alcoholic liver illness are the commonest causes of cirrhosis, adopted by nonalcoholic steatohepatitis and persistent hepatitis B (Chapters 140 and 143). Other causes of cirrhosis include cholestatic and autoimmune liver diseases, such as primary biliary cholangitis (Chapter 146), primary sclerosing cholangitis (Chapter 146), autoimmune hepatitis (Chapter 140), and metabolic illnesses, similar to hemochromatosis, Wilson disease, and 1antitrypsin deficiency (Chapter 137). When all potential causes have been investigated and excluded, cirrhosis is taken into account "cryptogenic. Hepatic stellate cells, which are known as Ito cells or perisinusoidal cells, are situated in the house of Disse between hepatocytes and sinusoidal endothelial cells. Normally, hepatic stellate cells are quiescent and serve as the principle storage site for retinoids (vitamin A). The sinusoidal endothelial cells themselves comprise large fenestrae (100 to 200 nm in diameter) that let the passage of huge molecules with molecular lots up to 250,000 daltons. B, on microscopic examination, liver sinusoids are organized, and vascular constructions are normally distributed. D, on microscopic examination, the structure is disorganized, and there are regenerative nodules surrounded by fibrous tissue. Decompensated cirrhosis is outlined by the development of ascites, variceal hemorrhage, encephalopathy or jaundice, all of that are consequences of portal hypertension (and the hyperdynamic circulatory state) and/or liver insufficiency. Cirrhosis and its sequelae cirrhosis portal hypertension ascites encephalopathy variceal hemorrhage 990. The growth of varices and ascites is a direct consequence of portal hypertension and the hyperdynamic circulatory state, whereas jaundice happens on account of an inability of the liver to excrete bilirubin. Ascites, in flip, can turn out to be complicated by an infection, which is called spontaneous bacterial peritonitis, and by functional renal failure, which is recognized as hepatorenal syndrome. Cirrhosis and its sequelae 991 Complications of Cirrhosis Portal Hypertension and the Hyperdynamic Circulatory State In cirrhosis, portal hypertension outcomes from both a rise in resistance to portal circulate and an increase in portal venous inflow. Early in the portal hypertensive course of, the spleen grows and sequesters platelets and other formed blood cells, thereby leading to hypersplenism. In addition, vessels that normally drain into the portal system, such because the coronary vein, reverse their flow and shunt blood away from the portal system to the systemic circulation. These portosystemic collaterals are insufficient to decompress the portal venous system and supply additional resistance to portal flow. As collaterals develop, a rise in portal blood influx, which results from splanchnic vasodilation, maintains the portal hypertensive state. This hyperdynamic circulatory state maintains portal hypertension, thereby resulting in the formation and progress of varices, and plays an necessary function in the improvement of all other issues of cirrhosis. Complications of cirrhosis outcome from portal hypertension or liver insufficiency. Complications of cirrhosis develop after the gradient will increase above 10 to 12 mm hg. Other indicators of liver insufficiency, such because the presence of encephalopathy or prolongation of the international normalized ratio, help decide the most probably contributor to hyperbilirubinemia (Chapter 138). The hyperdynamic circulatory state ultimately ends in high-output coronary heart failure with decreased peripheral utilization of oxygen, a complication that has been referred to as cirrhotic cardiomyopathy. Vasodilation at the level of the pulmonary circulation results in arterial hypoxemia, the hallmark of hepatopulmonary syndrome. Normal pulmonary capillaries are eight �m in diameter, and red blood cells (slightly lower than 8 �m) move via them one cell at a time, thereby facilitating oxygenation. In hepatopulmonary syndrome, the pulmonary capillaries are dilated as much as 500 �m, so passage of purple cells by way of the pulmonary capillaries may be many cells thick. However, because these factors result in endothelial proliferation, vasoconstriction, in situ thrombosis, and obliteration of vessels, irreversible pulmonary hypertension ensues. As the disease progresses, portal stress increases and liver operate worsens, thereby ensuing within the development of ascites, portal hypertensive gastrointestinal bleeding, encephalopathy, and jaundice. Progression to death could additionally be accelerated by the development of different issues, such as recurrent gastrointestinal bleeding, renal impairment (refractory ascites, hepatorenal syndrome), hepatopulmonary syndrome, and sepsis (spontaneous bacterial peritonitis). Transition from a compensated to a decompensated stage happens at a fee of approximately 5 to 7% per 12 months. The median time to decompensation, or the time at which half the sufferers with compensated cirrhosis will turn out to be decompensated, is about 6 years. Varices and Variceal Hemorrhage the complication of cirrhosis that outcomes most directly from portal hypertension is the development of portal-systemic collaterals, the most related of which are people who kind by way of dilation of the coronary and gastric veins and constitute gastroesophageal varices. Development of a hyperdynamic circulatory state leads to additional dilation and growth of varices and finally to their rupture and variceal hemorrhage, some of the dreaded complications of portal hypertension. Tension in a varix determines variceal rupture and is directly proportional to variceal diameter and intravariceal strain and inversely proportional to variceal wall thickness. Cardiopulmonary Complications Ascites and Hepatorenal Syndrome Ascites, which is the accumulation of intraperitoneal fluid, in cirrhosis is secondary to sinusoidal hypertension and retention of sodium. Cirrhosis results in sinusoidal hypertension by blocking hepatic venous outflow each anatomically by fibrosis and regenerative nodules and functionally by increased postsinusoidal vascular tone. Similar to the formation of esophageal varices, a threshold hepatic venous pressure gradient of 12 mm Hg is needed for the formation of ascites. In addition, retention of sodium replenishes the intravascular quantity and permits the continual formation of ascites. With development of cirrhosis and portal hypertension, vasodilation is extra pronounced, thereby leading to additional activation of the renin-angiotensin-aldosterone and sympathetic nervous systems and resulting in further sodium retention (refractory ascites), water retention (hyponatremia), and renal vasoconstriction (hepatorenal syndrome). Bacterial translocation, or the migration of micro organism from the intestinal lumen to mesenteric lymph nodes and other extraintestinal sites, is the main mechanism implicated in spontaneous bacterial peritonitis. Impaired native and systemic immune defenses are a significant factor in promoting bacterial translocation and, together with shunting of blood away from the hepatic Kupffer cells by way of portosystemic collaterals, enable a transient bacteremia to become more prolonged, thereby colonizing ascitic fluid. Spontaneous bacterial peritonitis occurs in patients with decreased ascites protection mechanisms, such as a low complement stage in ascitic fluid. Another factor that promotes bacterial translocation in cirrhosis is intestinal bacterial overgrowth attributed to a lower in small bowel motility and intestinal transit time. Infections, notably from gramnegative micro organism, can precipitate renal dysfunction by way of worsening of the hyperdynamic circulatory state. Encephalopathy Hepatic encephalopathy is brain dysfunction brought on by liver insufficiency, portosystemic shunting, or each. In cirrhosis, ammonia accumulates within the systemic circulation because of shunting of blood via portosystemic collaterals and decreased liver metabolism. Ammonia leads to upregulation of astrocytic peripheral-type benzodiazepine receptors, essentially the most potent stimulants of neurosteroid production. Neurosteroids are the major modulators of -aminobutyric acid, which results in cortical melancholy and hepatic encephalopathy. Other toxins, such as manganese, additionally accumulate in the mind, notably the globus pallidus, where they result in impaired motor perform. Other yet-to-be-elucidated toxins may also be concerned in the pathogenesis of encephalopathy. Jaundice Jaundice (Chapter 138) in cirrhosis is a reflection of the lack of the liver to excrete bilirubin and is due to this fact the results of liver insufficiency. Nonspecific fatigue, weight reduction, decreased muscle mass, decreased libido, or sleep disturbances could be the only complaints. Cirrhosis and its sequelae 993 Decompensated Cirrhosis At this stage, there are indicators of decompensation: ascites, variceal hemorrhage, jaundice, hepatic encephalopathy, or any combination of these findings. Ascites, which is essentially the most frequent sign of decompensation, is current in 80% of sufferers with decompensated cirrhosis. Nevertheless, hyponatremia is a marker of the severity of cirrhosis and is related to poorer high quality of life and the event of hepatic encephalopathy. Hepatorenal syndrome is a kind of prerenal kidney harm that happens in sufferers with cirrhosis and ascites. Hepatorenal syndrome is split into two sorts based on medical traits and prognosis. Type 1 hepatorenal syndrome is quickly progressive acute kidney damage by which the rise in serum creatinine concentration occurs within a 2-week interval. Patients with hepatorenal syndrome usually have tense ascites that responds poorly to diuretics, however no particular signs or signs typify this entity. About one third of cirrhotic patients are admitted for bacterial infection or acquire a bacterial an infection throughout hospitalization, the most common being spontaneous bacterial peritonitis. The two most necessary predictors of the development of bacterial an infection are the severity of liver disease and admission for gastrointestinal hemorrhage. The most frequent scientific manifestations of spontaneous bacterial peritonitis are fever, jaundice, and stomach ache. Variceal Hemorrhage Spontaneous Bacterial Peritonitis Gastroesophageal varices are current in approximately 50% of sufferers with newly diagnosed cirrhosis. The prevalence of varices correlates with the severity of liver illness and ranges from 40% in Child A cirrhotic sufferers (Table 144-2) to 85% in Child C cirrhotic patients. Both the development of varices and the growth of small varices happen at a fee of seven to 8% per yr. The incidence of a primary variceal hemorrhage in sufferers with small varices is about 5% per 12 months, whereas medium and huge varices bleed at a fee of approximately 15% per year. Large varices, extreme liver disease, and pink wale markings on varices are independent predictors of variceal hemorrhage. Bleeding from gastroesophageal varices may be manifested as overt hematemesis, melena, or each (Chapter 126). Ascites and Hyponatremia Hepatic Encephalopathy Ascites is the commonest reason for decompensation in cirrhosis and occurs at a rate of seven to 10% per yr. The most frequent symptoms associated with ascites are elevated stomach girth, which is often described by the affected person as tightness of the belt or garments across the waist, and recent weight acquire. Hyponatremia, which is defined as a serum sodium focus beneath one hundred thirty mEq/L (Chapter 108), is present in about 25% of patients with cirrhosis and ascites. Hepatic encephalopathy related to cirrhosis is of gradual onset and barely fatal. It is manifested as a large spectrum of neurologic and psychiatric abnormalities ranging from subclinical alterations to coma. On bodily examination, early phases could reveal solely a distal tremor, however the hallmark of overt hepatic encephalopathy is the presence of asterixis (Chapter 145). In addition, patients with hepatic encephalopathy might have sweet-smelling breath, a characteristic termed fetor hepaticus. Clubbing of the fingers, cyanosis, and vascular spiders may be seen on physical examination. Hepatopulmonary syndrome is present in roughly 5 to 10% of patients awaiting liver transplantation. Portopulmonary hypertension is manifested as exertional dyspnea, syncope, and chest pain. On examination, an accentuated second sound and proper ventricular heave are prominent (Chapter 75). The diagnosis of cirrhosis must be considered in any patient with chronic liver disease. In asymptomatic patients with compensated cirrhosis, typical indicators of cirrhosis is in all probability not present, and the physical examination and laboratory test findings may be entirely normal. The prognosis might often require histologic confirmation by liver biopsy, which is the "gold commonplace" for the analysis of cirrhosis. However, liver biopsy is an invasive procedure topic to sampling error, and the presence of cirrhosis can typically be confirmed noninvasively by a mixture of serum biomarkers, imaging methods, and measurements of liver stiffness.
Syndromes
- A woman is responding to fertility treatment
- Partial webbing or fusing of fingers or toes
- Heart disease
- Itching
- Lung abscess
- Pitting edema leaves a dent in the skin after you press the area with a finger for about 5 seconds. The dent will slowly fill back in.
- Increased feeling of cold
Diagnosis in turn requires appropriate use of laboratory testing informed by the history allergy forecast tacoma buy deltasone overnight delivery, physical examination allergy symptoms to kerosene generic 20mg deltasone mastercard, and prevalence of ailments within the population relevant to the affected person allergy medicine makes me drowsy buy discount deltasone 10mg on line. After an outline of the fundamental physiology regulating pink cell manufacturing allergy forecast santa fe buy deltasone canada, an strategy to anemia is outlined allergy treatment center kelapa gading buy deltasone with paypal, based on classification by the reticulocyte response to anemia and further refined by division into normocytic allergy zantac purchase deltasone 5 mg with amex, microcytic, and macrocytic anemia syndromes. In addition, particular anemia syndromes are discussed together with methemoglobinemia, anemia of renal insufficiency, anemia of liver illness, anemia of endocrine deficiencies, physiologic anemia of being pregnant, and unexplained anemia of aging. The treatment for acute methemoglobinemia is methylene blue 1 to 2 mg/kg, although larger doses up to 6 to 7 mg/kg may be required. The major regulator of red cell production is the effectiveness of oxygen supply. This crucial need could clarify why hemoglobin focus or hematocrit are controlled in a relatively slender regular vary as compared to the white blood depend or platelet count, where the higher restrict of normal may be two or 3 times the lower restrict of regular. The mediator that interprets peripheral oxygen must pink cell production is the hormone erythropoietin. After start, the predominant physiologic site of erythropoietin manufacturing is the kidney, though the liver retains some limited capacity for erythropoietin manufacturing, and neoplasms arising from different tissues and organs might secrete erythropoietin in an unregulated method. Erythropoietin binds to particular receptors on erythroid progenitors within the marrow resulting in elevated pink cell manufacturing. When correction of anemia normalizes the oxygen rigidity within the renal cortex, erythropoietin production falls back to basal levels. Ambient hypoxia or underoxygenation of the blood by a rightto-left cardiopulmonary shunt also leads to erythropoietin manufacturing. This causes the erythrocytosis seen in dwellers at high altitudes and in people with uncorrected cyanotic coronary heart disease. Red cell manufacturing has some feedback regulation of iron availability through the erythroferrone/hepcidin/ferroportin axis (Chapter 150). ApproAch to the AnemiAs 1029 failure of the palmar creases to become extra distinguished when the extended fingers are pushed down, extending the palm, typically indicates a hemoglobin no larger than 7 to eight g/dL. Tachycardia and a systolic ejection murmur might develop on account of anemia and cardiovascular lodging to it. Peripheral edema may be occasionally seen with reasonably severe anemia: this may mirror a mixture of high output coronary heart failure and loss of oncotic pressure associated with fewer blood cells. On rare events, retinal hemorrhages may be seen on fundoscopic examination in severe anemia. All of those vascular and cardiac manifestations of anemia will resolve with correction of anemia. Anemia of fast onset, as may be seen with huge acute hemolysis or with acute blood loss, is more more likely to be symptomatic than anemia from purple cell underproduction or from gradual gastrointestinal blood loss. Preservation of blood volume and cardiovascular accommodation are likely the reasons that sufferers, even the elderly, with slow onset anemias such as B12 deficiency are traditionally reported to turn out to be symptomatic at much decrease hemoglobin concentrations or hematocrits than patients with iron deficiency anemia from blood loss. A person with coronary artery illness or persistent obstructive lung disease is more likely to turn into symptomatic than an anemic particular person with out those issues who has the same hemoglobin focus. Palpitations or a way of the heart racing or pounding might occur, representing a extra fast coronary heart price and increased ejection fraction to find a way to keep oxygen supply. Symptomatology in anemia syndromes that develop as a consequence of some other illness (such as the anemia of inflammation in affiliation with rheumatoid arthritis) will most likely be dominated by the symptoms of the related disease. Pica, the need to eat nonnutritive substances such as ice, may be very specific to iron deficiency. Pallor can even occur in other conditions associated with shunting of blood away from the periphery to the critical organs. In the evaluation of anemia, pallor of the conjunctival mucosa or the creases within the palm are extra particular than pallor in other sites. Pallor of the conjunctival mucosa generally indicates a hemoglobin concentration lower than 9 g/dL; and Hematocrit, purple blood cell depend, and hemoglobin focus require adjustment to common items for red cell indices calculations. Certain bodily findings could assist information the analysis of anemia focus by offering clues to particular syndromes, underlying problems, or bleeding (Table 149-5). Petechiae, purpura, or thrush counsel abnormalities of the platelets or white cells and raise the risk of a generalized marrow dysfunction not restricted to the erythroid lineage. Frontal bossing (prominence of the brow as a result of expansion of red marrow in the skull) is seen in congenital hemolytic anemias but is often a regular variant; generally, adults with hemolytic anemia and this bodily finding have had their analysis defined earlier in life. The neurologic findings of B12 deficiency generally require a extra thorough examination than is part of the routine bodily examination (Chapter 155). Duration of anemia assists in distinguishing congenital from chronic or acute causes. Because iron deficiency is the most common etiology of anemia in scientific drugs, dietary historical past (vegetarian or vegan) and a history of blood loss should all the time be pursued. In women, this must also embody asking about variety of earlier pregnancies and whether iron supplementation was used in the course of the being pregnant. Every child delivered at term represents an investment of 800 mg of maternal iron (Chapter 150). A historical past of cholelithiasis in early maturity is suggestive of congenital hemolytic issues. A historical past of rheumatic or continual inflammatory issues raises the potential of the anemia of inflammation (Chapter 150). A historical past of petechiae or simple bruising or a history of recurrent infection raises the potential of a hematopoietic disorder not limited to the erythroid lineage. A history of a specific diagnosis, similar to sickle cell anemia or thalassemia, is obviously useful. Similarly, a historical past of members of the family with episodes of jaundice following minor diseases suggests a congenital hemolytic the same old full blood count supplied by automated cell counters contains quite a lot of instantly measured and calculated parameters, which at a minimum embody the white blood cell depend, the red blood cell depend, the hemoglobin concentration and hematocrit, the platelet rely, and the red cell indices described below. Many automated counters also present a differential white blood count and a semiquantitative description of purple cell abnormalities. Decreased counts of white blood cells and platelets are discussed in Chapters 158 and 163, respectively. Clinicians ought to turn out to be acquainted with the traditional values particular to the laboratories they use. The hematocrit and purple cell counts are concentrations as is the hemoglobin concentration, which signifies that a change within the plasma volume can elevate them or decrease them relative to the actual complete body red cell volume. An instance of an anemia (significant reduction in the hemoglobin focus or hematocrit) related to a standard or slightly elevated pink cell volume happens in the second trimester of normal being pregnant. In contrast, an elevated hemoglobin concentration or hematocrit with a traditional or decreased purple cell quantity can be seen in dehydration or the capillary leak syndrome Red cells can also be described by parameters called purple cell indices, which are routinely calculated by most electronic cell counters. Red blood cell parameter determinations will vary between laboratories depending upon tools used and on the inhabitants serving as the basis for the traditional range. For example, the traditional pink cell values among sufferers dwelling at excessive altitude are greater than these in normal subjects at sea level because of decrease ambient oxygen pressure driving larger erythropoietin production. Normal values are completely different between newborns, youngsters, and adults and between women and men after puberty. The distinction in regular hemoglobin concentration, hematocrit, and pink cell rely between grownup men and women is attributed to the action of testosterone in sensitizing erythroid progenitors to erythropoietin. Reticulocyte Count Red cells newly released from the bone marrow that have shed their nuclei but nonetheless comprise some nuclear materials within the cytoplasm are known as reticulocytes. Reticulocytes have been traditionally measured by way of supravital staining on contemporary smears, however now are most frequently measured by circulate cytometry know-how included into electronic blood counters. On the routine Wright-Giemsa� stained peripheral blood smear, reticulocytes are barely larger than pink cells, have little or no central pallor, and have a more grayish (polychromatic) tinge to the cytoplasm. The reticulocyte activity in a particular specimen can be expressed in a wide selection of methods (Table 149-3). All are based mostly on the principle that the reticulocyte response of the marrow to anemia varies with the diploma of anemia. The uncorrected reticulocyte count, sometimes referred to as the reticulocyte percentage, represents the percentage of purple blood cells that are reticulocytes. The different reticulocyte parameters characterize an effort to regulate this uncorrected value for the diploma of anemia. The simplest and most common adjustment is to express the reticulocyte depend as absolutely the reticulocyte rely, which is the reticulocyte percentage multiplied by the purple blood cell count. Reticulocyte counts are helpful within the preliminary approach to anemia in distinguishing anemias because of underproduction of purple cells from these associated with enough or overproduction however shortened survival within the circulation. During therapy of anemia, increases in the reticulocyte rely can predict response to therapy prior to increments in the hemoglobin concentration or hematocrit. Alternately, failure of the reticulocyte count to increase at the expected time can predict failure of present therapy and dictate a change of method. In congenital hemolytic anemias, the morphologic modifications characteristic of purple cell membrane abnormalities could also be seen (spherocytes, elliptocytes, and so forth. The "bite" and "blister" red cells found in hereditary defects of purple cell oxidative metabolism are unlikely to be appreciated except by direct examination by a clinician. The finding of a dimorphic red cell population is a major clue to this disorder however may be seen in partially treated iron deficiency. Macro-ovalocytes and hypersegmented neutrophils are a extremely specific clue to B12 deficiency. Bone marrow aspiration and biopsy are required for the analysis of many major marrow problems giving rise to anemia. Disorders that require bone marrow examination for diagnosis these days are aplastic anemia and pure red cell aplasia, myelodysplastic syndromes, and anemias associated with marrow alternative (lymphoma, leukemia, myelofibrosis, myeloma, or metastatic cancer). Bone marrow examination for the analysis of anemia should include each aspiration and biopsy, and routinely embody Prussian blue staining for evaluation of iron stores and attainable detection of ringed sideroblasts. Flow cytometry to phenotype myeloid or lymphoid/plasma cell populations must also be carried out, as ought to normal cytogenetics, when suspecting a clonal dysfunction. Molecular research for parvovirus in instances of potential pure pink cell aplasia can be carried out on peripheral blood. A more recent discovery is that clonal abnormalities of hematopoiesis may be recognized on peripheral blood molecular testing, particularly in the elderly. This is an acceptable and intellectually legitimate method at any time, but significantly in the inpatient or hospitalbased clinic settings. In the ambulatory follow setting for many internists, third-party payers may mandate that laboratory studies be sent to outside reference laboratories. The consequence of such policies is that blood count and reticulocyte depend results will not be out there on the day of the visit, and private evaluation of the blood smear could also be challenging. Iron deficiency anemia and the anemia of inflammation (also called anemia of chronic disease) can both be identified by these tests and are the 2 most typical etiologies of anemia (Chapter 150). Bone Marrow Examination Anemia associated with elevated reticulocyte manufacturing after adjustment for anemia suggests the presence of either blood loss or hemolysis. There are certain conditions the place bleeding or hemolysis will not be related to an appropriate reticulocyte response; these usually indicate some concurrent restriction on purple cell production corresponding to iron or folate deficiency. Hypovolemia and loss of the oxygen-carrying capacity of pink cells might impair oxygen delivery to tissues. Blood flow preferentially shunts to the crucial organs like the guts, mind, kidneys, and liver and is diverted away from the pores and skin and musculature. In the preliminary setting of acute blood loss, plasma and red cells are depleted of their similar relative ratio. As the intravascular quantity is expanded, either rapidly with exogenous, intravenous colloid or crystalloid in the setting of trauma, or extra slowly by endogenous redistribution of plasma from the extravascular house, the hematocrit and hemoglobin concentration will begin to transfer downward over hours to days to reveal the true extent of lack of circulating red cell volume. In this setting, due to this fact, the diploma of blood loss is initially underestimated by the blood counts. Further complicating the scenario in the case of acute trauma is cytokine activation and the "coagulopathy of trauma. Bleeding into the gastrointestinal tract can lead to hematemesis, melena, and/or hematochezia, relying on the situation and rate of bleeding. Bleeding may be associated with reactive thrombocytosis and occasionally leukocytosis. The management of massive blood loss is by transfusion (Chapter 167) and correction of the purpose for bleeding. The reticulocyte count stays appropriately elevated until iron becomes depleted by its utilization for elevated erythropoiesis, at which era the reticulocyte response decreases and the hemoglobin concentration and hematocrit start to drift downward. In this sense, some reduction in pink cell survival is an element in lots of hematologic syndromes. Decreased pink cell survival is a part of the anemia observed in renal disease, the anemia of irritation, and the anemia of liver disease (distinct from spur cell anemia). Microangiopathic hemolytic morphology is often seen in disseminated intravascular coagulation. The issues discussed here are those in which the first etiology of anemia is hemolysis, with further details concerning the particular disorders of hemolysis in Chapters 151, 152, 153, and 154. Table 149-7 outlines laboratory studies that elevate suspicion of a hemolytic anemia and those who verify it. The distinction between extravascular hemolysis (which includes hemolysis within the spleen) and intravascular hemolysis is helpful in understanding these disorders on the pathophysiologic level. Table 149-8 lists causes of hemolysis, utilizing a well-liked classification that separates etiologies which may be (1) completely external to the red cell. The enzymatic defects producing hemolysis are typically associated to oxidative metabolism and notably to oxidative stress similar to that induced by medications. Specific syndromes of hemolytic anemias are discussed in Chapters 151 by way of 154. The objective of this part is to define a general approach to hemolytic anemias that can then be expanded upon within the chapters dedicated to particular syndromes. In hemolytic anemia, the examination of the peripheral smear is extraordinarily essential and more likely to yield important info.
Purchase deltasone online from canada. Am I Allergic to Eye Shadow? : Eye Treatments.
References
- Terada, N., Arai, Y., Kinukawa, N. et al. Risk factors for renal cysts. BJU Int 2004;93:1300-1302.
- Urbanowicz JH, Shaaban MJ, Cohen NH, et al: Comparison of transesophageal echocardiographic and scintigraphic estimates of left ventricular end-diastolic volume index and ejection fraction in patients following coronary artery bypass grafting, Anesthesiology 72:607, 1990.
- Burr ML, Fehily AM, Gilbert JF, et al. Effects of changes in fat, fish and fibre intakes on death and myocardial reinfarction: diet and reinfarction trial. Lancet 1994;343: 1454.
- Wooley JA. Characteristics of thiamin and its relevance to the management of heart failure. Nutr Clin Pract 2008;23:487-493.
- Longhi A, Errani C, Gonzales-Arabio D, et al. Osteosarcoma in patients older than 65 years. J Clin Oncol 2008;26(33):5368-5373.
- Wehnert J, Sage S: Comparative investigations to the action of Mictonorm (propiverin hydrochloride) and Spasuret (flavoxat hydrochloride) on detrusor vesicae, Z Urol Nephrol 82:259, 1989.
- Clements JL, Cox GW, Torres WE, et al. Cervical esophageal webs - a roentgen-anatomic correlation. AJR 1974; 121:221-231.