
Dr James Down
- Consultant in Intensive care and Anaesthesia
- University College Hospital
- London
Fatal mucormycosis presenting as an appendiceal mass with metastatic spread to the liver throughout chemotherapy-induced granulocytopenia medicine reminder discount generic actonel uk. This chapter reviews appendiceal mucinous tumours 4 medications list order actonel 35mg free shipping, adenocarcinomas treatment 5ths disease cheap actonel 35 mg line, endocrine tumours symptoms of diabetes buy 35 mg actonel with amex, goblet cell carcinoids, lymphomas and mesenchymal tumours, and ends with a quick discussion of metastatic tumours to the appendix. Abdominal pain that mimics acute appendicitis or an stomach mass (sometimes ovarian) is the most typical presentation [3,6,7,9], however a big quantity are discovered by the way. The mucinous epithelial cells are columnar and mucin wealthy and have elongated, mildly hyperchromatic nuclei, nuclear pseudo-stratification, uncommon mitoses and apoptotic nuclear debris [3,9,10]. Cystic tumours are lined by mucinous epithelium that can be partly villous, flat or attenuated. The prognosis of low grade appendiceal mucinous neoplasms depends on the presence or absence of epithelial cells outdoors the appendix. Tumours which have ruptured could also be related to mucin spillage in to the peritoneal cavity. The presence of epithelial cells in the extra-appendiceal mucin, even if restricted and confined to the best lower quadrant, will increase the chance of recurrence [12,13]. Colonoscopy is usually advised in sufferers found to have appendiceal mucinous tumours, because of a major association with synchronous and metachronous colorectal neoplasia. Adenocarcinoma Adenocarcinoma of the appendix is uncommon; Collins discovered an incidence of 0. Patients are normally in their fifth to seventh decades [15�18] and have symptoms of appendicitis, though they might current with a palpable mass, obstruction, gastrointestinal bleeding or signs referable to metastases [7,16�20]. In common, appendiceal adenocarcinomas manifest as either cystic mucinous tumours which would possibly be prone to rupture and spread to the ovaries and peritoneum or intestinal-type carcinomas that infiltrate the appendiceal wall and metastasise to lymph nodes and the liver. Mucinous adenocarcinoma accounts for about 40% of appendiceal adenocarcinomas [18]. Appendiceal nonmucinous carcinomas show a variety of morphology of the invasive element. In some instances, the tumour has an look equivalent to colonic adenocarcinoma with malignant glands lined by columnar epithelium. In different cases, the malignant glands are tubular in shape, lined by cuboidal epithelium and associated with modest amounts of extracellular mucin. Signet-ring cell carcinoma is uncommon in the appendix and has a poor prognosis as a end result of fast dissemination inside the peritoneal cavity [21]. The reported 5-year survival price for sufferers with appendiceal adenocarcinoma ranges from 18. Patients with mucinous adenocarcinomas fare higher than these with non-mucinous adenocarcinomas [17,19]. Virtually all authors agree that proper hemicolectomy is indicated for invasive adenocarcinoma, both to obtain complete tumour resection and to stage the tumour by examining the proper colic lymph nodes [17,19,20]. Furthermore, hemicolectomy provides improved 5-year survival rates 492 Appendix relative to appendectomy [10,17,20]. Some authors advocate oophorectomy in women both for staging purposes and to remove a website where tumour frequently recurs [17,19]. Pseudomyxoma peritonei Pseudomyxoma peritonei refers to the accumulation of mucin and mucinous epithelial cells within the peritoneal cavity, secondary to peritoneal spread of a mucinous neoplasm. Peritoneal mucinous tumours with high grade cytological atypia and extra mobile, complex, epithelial proliferations are usually related to either severely atypical mucinous neoplasms or frankly invasive mucinous carcinomas [4,9]. The mucinous peritoneal deposits accumulate in the larger omentum, undersurface of the proper hemidiaphragm, pelvis, proper retrohepatic area, left stomach gutter and ligament of Treitz [25]. These peritoneal tumours derived from an appendiceal or intestinal mucinous adenocarcinoma and had been characterised by parenchymal organ invasion and lymph node metastases. Historically, remedy was considered palliative and consisted of serial surgical tumour debulking until abdominal adhesions precluded additional debulking and the affected person died of bowel obstruction. Sugarbaker and colleagues [27] advocate an approach that goals for treatment and consists of peritonectomy procedures to obtain complete cytoreduction, coupled with intra-peritoneal chemotherapy. However, these protocols are associated with vital morbidity and others have reported comparable outcomes with extra conservative approaches [28]. Hyperplastic polyp, diffuse mucosal hyperplasia and sessile serrated adenoma Hyperplastic polyps occur hardly ever within the appendix and are much like hyperplastic polyps elsewhere within the colon. They are small, localised areas by which the crypts are elongated and lined by mucinous epithelium, which contains a mixture of goblet cells interspersed amongst mucinous cells with smaller mucin vacuoles. The crypt lumens appear serrated, predominantly towards the luminal surface of the lesion. Hyperplastic polyps of the appendix are frequently incidental findings however might happen in sufferers with signs of appendicitis. Diffuse mucosal hyperplasia uncommonly impacts the appendix and is normally an incidental finding [3]. A collection of 10 serrated adenomas within the appendix [31] found invasive carcinoma in four instances, suggesting a excessive chance of progression in these lesions. Colonic-type tubular adenomas Localised polypoid adenomas of the sort seen within the colon (see Chapter 37) are uncommon within the appendix [32]. The histological look of these polyps is identical to tubular adenomas in the colon. Endocrine (carcinoid) tumours Appendiceal endocrine (carcinoid) tumours account for approximately 18. Most are discovered incidentally [36,40], though occasional tumours present with appendicitis or recurrent stomach pain [34,41], particularly in youngsters [37,38]. Approximately 75% of them are <10 mm in diameter and approximately 5% are >20 mm [34,36,42]. Tumour cells are uniform, with modest amounts of eosinophilic, finely granular cytoplasm. Infiltration of the meso-appendix happens in as a lot as 27% of circumstances [35,41,42], although that is proportionate to tumour dimension. These tumours stain unreliably for chromogranin A however specific chromogranin B and synaptophysin [45,46]. The frequency of metastasis Tumours of the appendix 495 is extremely depending on tumour measurement, with 0% for tumours <10 mm, 3�6. Patients with native illness have a 5-year survival rate of 92�100%, these with regional metastasis 81% and those with distant metastasis 31% [36,forty nine,50]. Investigators making an attempt to outline which features of appendiceal carcinoid tumours predict behaviour have found only tumour size to be related: tumours <20 mm occasionally metastasise and people <10 mm are essentially benign [34,51]. Factors which were dismissed as prognostic elements are depth of invasion, location of the tumour within the appendix, perineural invasion, lymphatic invasion and the presence of serosal tumour [42,51]. Studies analyzing the importance of invasion of the meso-appendix have yielded conflicting outcomes. Some authors report an increased probability of metastatic illness in sufferers with meso-appendiceal infiltration independent of tumour dimension [52], whereas others report that meso-appendiceal invasion has no impact on prognosis in tumours <20 mm [35,53]. Simple appendectomy is healing for lesions <10 mm if the margin of resection is unfavorable for tumour. The lesions are sometimes situated in the submucosa and muscularis propria of the appendiceal tip, span a few millimetres and are just about at all times an incidental finding found on microscopic examination. Chromogranin immunohistochemistry is variable and weak [45,fifty four,55] but the tumours are usually constructive for synaptophysin. They most often have an result on sufferers in their fifth decade with an equal sex distribution [56]. The tumours most often present as appendicitis [57,58], though they are often an incidental finding or in women present with ovarian metastases [59�62]. Grossly, these tumours usually seem as circumferential thickening of the appendix and are only recognised on microscopic examination. Tumour dimension is, subsequently, tough to decide in lots of instances but averages 20 mm [56]. Histological examination shows circumferential infiltration of the appendix by a tumour that appears to come up from the bottom of crypts with no recognisable precursor lesion. Most tumour cell clusters lack lumina [63]; these with lumina resemble intestinal crypts. Immunohistochemistry for chromogranin and synaptophysin shows staining of occasional endocrine cells within the tumour clusters [67]. Isaacson demonstrated that many tumours show staining for IgA, secretory element and lysozyme, typical of intestinal crypt cells. Features that predict a worse prognosis include tumour extension past the appendix at presentation, atypical histological options and more than two mitoses per 10 excessive power fields [70].
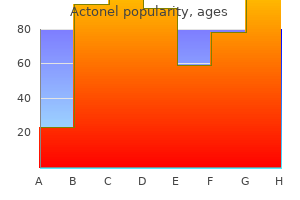
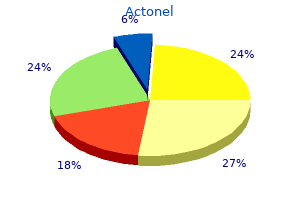
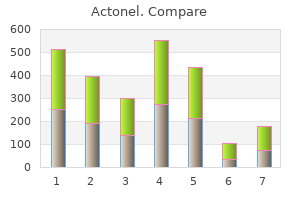
alfacalcidol (Vitamin D). Actonel.
- What is Vitamin D?
- Low blood calcium levels because of a low parathyroid thyroid hormone levels.
- Reducing the risk of rheumatoid arthritis in older women. Bone loss in women with a condition called hyperparathyroidism.
- Preventing breast cancer.
- Treating conditions that cause weak and painful bones (osteomalacia).
- Reducing the risk of multiple sclerosis (MS).
- Rickets.
- Reducing bone loss in people taking drugs called corticosteroids.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96892
Granulomatous inflammation could correlate with low virulence teams and suppurative irritation with high virulence instances [85] treatment variance order 35mg actonel with amex. The formation of granulomas 6 mp treatment buy actonel online pills, usually of geographical shapes and confluent medications for bipolar purchase genuine actonel, then supervenes medicine reviews order actonel without prescription. These usually have a central necrotic zone infiltrated by polymorphs and forming a micro-abscess, surrounded by epithelioid cells and histiocytes. This sample of necrotising granulomatosis is comparable to that seen in different infective lymphadenitides, most notably cat scratch fever and lymphogranuloma venereum. Yet, with immunohistochemistry, it has been proven that the granulomas are composed of quite a few histiocytes along with scattered T lymphocytes whereas B cells had been rare [86]. The thickening of the ileal wall is apparent with ulceration of the mucosa over the hyperplastic lymphoid tissue. When the disease is more pronounced, there may be proof of deep ulceration and submucosal oedema, though involvement of the muscularis propria is uncommon. Furthermore small intestinal bacterial overgrowth could cause elevated antigliadin antibody ranges in small intestinal luminal secretions and therefore has the potential to trigger over-diagnosis of coeliac disease. Within the immigrant neighborhood, the best incidence of gastrointestinal involvement happens within the years quickly after arrival in the west. In a examine from Hong Kong, the ileocaecal region was involved in 86% of sufferers [102]. In the primary, ingested bacilli (from contaminated milk) are believed to arrange a major reaction within the intestinal wall or in mesenteric lymph nodes. In the second, the source is swallowed infected sputum from a primary lung lesion or an extra oral dose of bacilli establishing a re-infection in an already sensitised individual. The latter used to be the more widespread form however, in newer studies, accounts for lower than half of all circumstances [100,103]. A further modality of development is haema- Other bacterial causes of enteritis Acute bacterial enteritis can further be caused by Aeromonads, Gram-negative, oxidase-positive micro organism and Klebsiella spp. In children, Aeromonads seem to be a comparatively widespread cause of acute self-limiting diarrhoea [90], whereas in older adults it could cause a extra chronic enterocolitis [91]. Although strictly not an enteritis, in that it often presents with an ileo-caecal continual inflammatory phlegmon, actinomycosis ought to always be thought-about in the differential diagnosis of continual active inflammatory pathology affecting the terminal ileum and proximal colon, particularly in girls utilizing an intrauterine contraceptive gadget. Bacterial overgrowth within the small gut Bacterial overgrowth is a clinical syndrome, presenting with malabsorption, weight reduction and diarrhoea [93]. Previous surgery, particularly gastrectomy [95], small intestinal dysmotility including diabetes mellitus [96], jejunal diverticulosis and Inflammatory disorders of the small intestine 325 togenous spread from energetic pulmonary illness, whereas direct extension from adjacent organs could be very uncommon. Areas of involvement, often multiple, are found with growing frequency from the jejunum to the ileum, being significantly frequent within the terminal ileum and ileo-caecal space [104]. This distribution follows the localisation of lymphoid tissue in the small gut. The appearances of the minimize surface of the affected bowel rely upon the stage of the illness. In extra persistent illness, caseation will not be a function and the pathology is dominated by dense fibrosis, with destruction of the traditional tissues of the bowel wall, together with the muscularis propria. The small bowel is a site of predilection for this opportunistic an infection and, general, the gastrointestinal tract is an early, possibly major, website of colonisation. Sometimes the changes are very refined with just scanty collections of foamy histiocytes within the lamina propria. The an infection is very uncommon, though the causative bacterium Tropheryma whipplei is ubiquitously present in the setting. Inflammatory disorders of the small intestine 327 loss (92% of the cases), diarrhoea (76%), migratory arthralgia of the large joints or, much less commonly, non-deforming oligoarthritis or polyarthritis (67%) and abdominal ache (55%). The illness has a propensity to systemic involvement with fever (38%), lymphadenopathy (60%), and cardiac (especially endocarditis), pulmonary and central nervous system involvement all nicely described. Some sufferers develop extreme symptoms of malabsorption, corresponding to ascites and peripheral oedema. The disease is most often recognized by small bowel (either duodenal or jejunal) biopsy. Whipple originally demonstrated rod-shaped structures inside the cytoplasm of macrophages [116]. The postulation that these structures were bacteria was supported by the primary successful remedy with antibiotics within the Fifties. The sequencing of the complete genome from two completely different strains elucidated its phylogenetic place as a G�C-rich Gram-positive actinomycete. The organism has been detected in saliva, subgingival plaque and stool samples [124]. It is, nonetheless, clear that the illness can be regarded as an an infection attributable to a Gram-positive actinomycete, associated with profound immunological defects that enable the survival of the micro organism within macrophages [126]. Macrophages present a persistently diminished capacity to degrade the intracellular organisms. These abnormalities correlate with the diminution of immunocompetent B cells, regardless of the massive histiocytic inflow [118,127]. However, none of these options supplies proof of a main immunological abnormality to explain a predilection to infection by T. It is still possible to reason that the an infection causes secondary immunological abnormalities, in prone individuals, which improve the pathological results of the an infection [119,125]. It has been instructed that glycosylation of the bacterium, an intracellular antigen-masking system, might impair antibodymediated immune recognition in sufferers [129]. At laparotomy, the affected small bowel serosa is lined by exudate and the intestine appears thickened, dilated and inflexible. Upper gastrointestinal endoscopy of the small gut is the primary diagnostic check of selection. To keep away from sampling errors, 5 biopsies must be taken from varied sites of the duodenum. Classic lesions show a level of villous blunting and villous atrophy with preservation of epithelial cells, whereas the lamina propria is significantly expanded by quite a few pale-staining histiocytes. Sarcoid-like granulomas may be observed in samples from different tissues, together with lung, abdomen and lymph nodes. In some cases gastrointestinal symptomatology and intestinal involvement is minimal or focal [133]. If just one take a look at, histochemistry or immunohistochemistry, is optimistic, the prognosis is tentative. If both exams are unfavorable, but scientific suspicion stays, other samples must be examined. Positive immunohistochemical outcomes have been noticed in central nervous system disease. Although tetracycline has been the mainstay of remedy, relapse is nicely described and due to this fact other antibiotic regimens, often combination therapies, at the moment are used. These have included penicillin and streptomycin and, more just lately, ceftriaxone followed by trimethoprim and sulfamethoxazole, the latter now being the beneficial remedy [118,138]. Relapses normally occur only some years after remedy and are accompanied by a re-emergence of viable micro organism. Some sufferers stay refractory to antibiotic remedy and will require each comprehensive antibiotic regimens and immunomodulatory therapy. Small intestinal infarction due to aspergillosis has been described after chemotherapy (in neutropaenic patients), and in transplant recipients [146�148]. Macroscopically fungal infections usually present with ulceration, irregular shaggy mucosal surfaces resembling pseudo-membranous enterocolitis or inflammatory plenty [143]. The affiliation of ulceration with intensive fungal involvement of intramural blood vessels can also be a feature of mucormycosis in the small bowel. Mucormycosis is an usually deadly fungal an infection, caused by the category Phycomycetes subdivided in to the genera Absidia, Mucor and Rhizopus. The an infection occurs most regularly in sufferers with haematological malignancies, transplanted sufferers receiving immunosuppression and sufferers with malnutrition or on desferrioxamine remedy for iron overload. In the gastrointestinal tract, the abdomen is probably the most frequent web site of involvement, adopted by the colon and small gut [150]. The fungal hyphae are characteristically broad and irregular, hardly ever septate, with right angle branching: these features assist to differentiate Mucor sp.
For a better understanding of cardiac toxicology symptoms west nile virus discount actonel 35mg amex, a triangle model of cardiac toxicity is offered in treatment enlarged prostate discount actonel 35 mg mastercard. In this mannequin hair treatment buy actonel cheap, complexity of the interplay between environmental stresses and the center medications on backorder discount 35mg actonel with amex, and the stability between myocardial protection and deleterious dose and time results are considered. First, it may be very important acknowledge that chemicals can lead to coronary heart failure without coronary heart hypertrophy. Second, a chemical can lead to activation of both protecting and harmful responses in the myocardium. Third, long-term toxicological responses usually end in maladaptive hypertrophy, which primes the guts for malignant arrhythmia, resulting in sudden cardiac dying or transition to heart failure. In the research of cardiac toxicology, the manifestations of cardiac toxicity in human patients and animal models are crucial parameters serving as indices of cardiac toxicity. These manifestations are expressed in the types of cardiac arrhythmia, hypertrophy, and heart failure. These abnormal modifications reflect myocardial practical alterations resulting from both acute and chronic cardiac toxicity. Although some modifications together with cardiac hypertrophy had been viewed as a compensatory response to hemodynamic adjustments in the past, newer research suggest that cardiac hypertrophy is a maladaptive process of the center in response to intrinsic and extrinsic stresses (van Empel and De Windt, 2004; Berenji et al. Cardiac hypertrophy is a threat issue for sudden cardiac dying and has a excessive potential to progress to overt heart failure. Therefore, a distinction between compensatory and maladaptive responses is critical for remedy of patients with toxicological cardiomyopathy. Heart Failure A traditional definition of coronary heart failure is the inability of the center to maintain cardiac output enough to meet the metabolic and oxygen calls for of peripheral tissues. This definition has been modified to embody changes in systolic and diastolic function that replicate specific alterations in ventricular function and abnormalities in a selection of subcellular processes (Piano et al. Therefore, an in depth analysis to distinguish right ventricular from left ventricular failure can present a better understanding of the nature of the heart failure and predicting the prognosis. Acute Cardiac Toxicity Acute cardiac toxicity is referred to as cardiac response to a single publicity to a excessive dose of cardiac toxic chemicals. For occasion, a single excessive dose of arsenic can lead to cardiac arrhythmia and sudden cardiac dying, which is straightforward to measure (Goldsmith and From, 1980). However, that a single oral dose of monensin (20 mg/kg) results in a diminished cardiac perform progressing to heart failure in calves requires a long-term observation; often a couple of months for clinical signs of coronary heart failure (van Vleet, et al. Chronic Cardiac Toxicity Chronic cardiac toxicity is the cardiac response to long-term exposure to chemical substances, which is often manifested by cardiac hypertrophy and the transition to coronary heart failure. About 25% of human sufferers with cardiomyopathy are categorized as having idiopathic cardiomyopathy. At least a portion of Cardiac Arrhythmia Cardiac rhythms underneath physiological conditions are set by pacemaker cells which would possibly be usually capable of growing spontaneous depolarization and answerable for generating the cardiac rhythm, the so-called automatic rhythm. A cardiac rhythm that deviates from the normal automatic rhythm is called these patients with idiopathic cardiomyopathy are because of chemical exposure. Recognition of chronic cardiac toxicity in the pathogenesis of cardiomyopathy is of clinical relevance, and this data can be used to stop and treat sufferers with toxicological cardiomyopathy. In the past, the center has been considered incapable of regenerating, so that cardiac injury within the type of cell loss or scar tissue formation was thought of everlasting damage to the center. However, evidence now signifies myocardial regeneration and recovery from cardiomyopathy. Cardiac toxic responses or injury at the moment are divided in to reversible and irreversible. Myocardial Degenerative Responses Myocardial cell demise, fibrosis (scar tissue formation), and contractile dysfunction are thought of as degenerative responses, which can lead to cardiac arrhythmia, hypertrophy, and heart failure. Both acute and chronic toxic stresses can result in irreversible degeneration, relying on whether or not the cardiac restore mechanisms are overwhelmed. Both apoptosis and necrosis happen in the strategy of myocardial cell death, which will be mentioned in the next section. Myocardial cell dying is accompanied by hypertrophy of the remaining cardiac myocytes so that within the hypertrophic coronary heart, the whole variety of cardiac myocytes is decreased however the dimension or volume of individual cells is elevated. During myocardial transforming after cell dying, not only is there a rise in the size of cardiac myocytes, but additionally cardiac fibrosis occurs. The actions of those enzymes are altered through the processes of fibrogenesis and fibrinolysis. Under toxic stress circumstances, the imbalance between fibrogenesis and fibrinolysis leads to enhanced fibrogenesis and excess collagen accumulation-fibrosis. Common chelating groups include hydroxamates, carboxylates, thiols, and phosphinyls. Thus, cell death would result in a everlasting loss of the entire variety of cardiac myocytes. However, this view has been challenged just lately due to the identification of cardiac progenitor cells (Anversa et al. These cells are characterised and proposed to be responsible for cardiac restore as a result of these cells can make myocytes and vascular constructions. They are self-renewing, clonogenic, and multipotent, as demonstrated by reconstitution of infarcted coronary heart by intramyocardial injection of cardiac progenitor cells or the local activation of those cells by progress components. One speculation is that when severe damage to cardiac progenitor cells occurs, the potential for recovery from severe cardiac harm can be restricted. The elimination of scar tissue or fibrosis within the myocardium up to now has been thought of impossible. Many toxic insults affect the capability of angiogenesis in the myocardium, so that cardiac ischemia occurs. The mixture of cardiac ischemia and the direct toxic insults to cardiomyocytes constitute synergistic injury to the center. During regeneration, coronary arterioles and capillary buildings are shaped to bridge the dead tissue (scar tissue) and supply vitamins for the survival of the regenerated cardiomyocytes. There is an orderly organization of myocytes throughout the myocardium and a well-defined relationship between the myocytes and the capillary community. This proportion is altered underneath cardiac toxic circumstances; either toxicological hypertrophy or diminished capillary formation can result in hypoperfusion of myocytes within the myocardium. Unfortunately, our understanding of the poisonous results on myocardial angiogenesis is proscribed. The problem related to whether or not toxicological cardiac lesions are reversible has not been explored. However, it might be speculated that there could be reversible and irreversible manifestations of the cardiac response to poisonous insults. With regard to this, poisonous effect on the capability of myocardial regeneration is a significant concern and myocardial regenerative toxicity determines the fate of toxicological cardiomyopathy reversible or irreversible. Myocardial Cell Death and Signaling Pathways Apoptosis and Necrosis Toxic insults set off a sequence of reactions in cardiac cells leading to measurable adjustments. However, extreme injuries will lead to cell demise within the modes of apoptosis and necrosis. If the cell survives the insults, structural and practical adaptations will take place. The loss of cardiac myocytes is a elementary part of myocardial damage, which initiates and aggravates cardiomyopathy. An important mode of myocardial cell loss is apoptosis, which has been demonstrated in coronary heart failure patients (Olivetti et al. Myocardial apoptosis has been proven to play an essential role in cardiac poisonous results induced by Adriamycin (Kang et al. Exposure of main cultures of cardiomyocytes to cadmium additionally induces apoptosis (El-Sherif et al. Many in vivo research have proven that only a really small share of myocardial cell populations undergo apoptosis underneath pathological situations. At first look, this number appears to be too insignificant to account for myocardial pathogenesis. Myocytes that undergo apoptosis are lost and will not be changed underneath toxicological conditions. Although the potential of myocardial regeneration has been recognized (Anversa et al.
Those exterior the ampulla are usually small and lack infiltrative development [97] medications quotes buy actonel with american express, whereas those at the ampulla have produced clinically obstructive results [96 medications ok for dogs cheap 35mg actonel with mastercard,98] medicine cat herbs cheap actonel 35 mg line. Gangliocytic paraganglioma this uncommon tumour has been the subject of a lot curiosity due to its unsure histogenesis symptoms nasal polyps discount 35mg actonel overnight delivery, its peculiar histological look and its virtually unique location within the periampullary portion of the duodenum. The tumour has been reported in patients aged 17�84 years, with a slight female predominance (1. Gangliocytic paragangliomas are generally solitary, sporadic lesions, though multiple tumours have been recorded [100]. Rare circumstances of gangliocytic paraganglioma of the jejunum have been reported, one arising in affiliation with pancreatic heterotopia [105]. Macroscopically, gangliocytic paragangliomas are usually polypoid, exophytic lesions that protrude in to the lumen of the gut. They measure up to 70 mm in diameter and present with haemorrhage, anaemia and/or duodenal or biliary obstruction. Grossly, the tumour is centred on the submucosa and there could also be focal ulceration. Amyloid could also be present in relation to the epithelioid cells and concentrically laminated psammoma bodies can also be discovered, particularly if the endocrine cells comprise somatostatin [109]. They are often organized in well-demarcated nests, reminiscent of the Zellballen of classic paragangliomas. Mitotic figures and necrosis are just about by no means seen, though a reasonable diploma of pleomorphism may be current. The three cellular parts intermingle with the normal easy muscle and small pancreatic ducts at the ampulla to produce a complex lesion. Two broad theories exist with regard to histogenesis: the primary proposes that they arise due to pancreatic maldevelopment [107]. This is supported by the frequent presence, throughout the tumour, of misplaced pancreatic tissue and the excessive incidence of immunoreactivity for pancreatic polypeptide and somatostatin. The second theory suggests a neoplastic lesion [108], with a posh triphasic progress sample. Rare stories of local lymph node deposits composed of the endocrine cell element, both alone [111] or with sparse spindle cell or ganglion cell elements [110], support this. An similar tumour happens within the cauda equina area [112], the origin of which is troublesome to clarify on the premise of pancreatic maldevelopment. Poorly differentiated endocrine carcinoma/small cell carcinoma Fewer than 30 circumstances of this uncommon and extremely aggressive periampullary tumour have been recorded within the literature, most presenting with obstructive jaundice, belly pain and weight loss, and followed by a quickly fatal course [114,115]. The tumours are small (20�30 mm), ulcerated or protuberant lesions which microscopically reveal sheets or nests of small, mitotically lively cells with round or oval hyperchromatic nuclei, scanty cytoplasm and foci of necrosis. Using haematoxylin and eosin (H&E) staining, they resemble both small cell carcinomas or massive cell endocrine carcinomas. Malignant lymphoma must be excluded by immunocytochemistry and metastatic tumours by medical examination and radiology. Localised tumours may be resectable and metastatic tumours might respond to chemotherapy [72,117]. Goblet cell carcinoid A few instances of this uncommon tumour have been reported inside the duodenum, both at the ampulla of Vater [118,119] or throughout the duodenal bulb [120]. Morphologically, these were small tumours that appeared equivalent histologically to their extra common counterparts in the appendix (see Chapter 30), being composed of small infiltrative nests of cytologically bland goblet cells, signet-ring cells and endocrine cells. By analogy with appendiceal goblet cell carcinoids, their prognosis should be intermediate between those of well differentiated endocrine tumours and adenocarcinomas of the duodenum. The neoplasm has an aggressive behaviour and dying normally results from widespread metastases [125]. One research showed lack of expression of p14, p15 and p16 in the 9p21 gene cluster [139]. Small tumours are sometimes found by the way submit mortem or at laparotomy whereas bigger neoplasms current with abdominal pain, intestinal obstruction or ischaemia from the native effects of the tumour. In addition, these tumours regularly result in a dense desmoplastic response of the mesentery, usually at a distance from the primary tumour; this may cause subacute or frank obstruction. Multiple tumours are associated with a youthful age of onset, an increased risk of carcinoid syndrome and a poorer prognosis [141]. This final finding appears to be according to the current view that multiple tumours could represent metastases as opposed to impartial major neoplasms. A recent research [142] confirmed an similar X-chromosomal inactivation sample in multiple tumours, implying a standard neoplastic clone. Palliative surgical procedure is individualised on a case-by-case basis: resection of an asymptomatic major tumour, even within the presence of liver metastases, is beneficial to prevent small bowel occlusion or native complications at a later stage [143]. The main lesions in the bowel wall range from barely palpable foci of thickening to nodules measuring up to 35 mms; hardly ever do the primary tumours exceed this dimension. Clinically, patients might current with intestinal obstruction, volvulus or ischaemia. It would appear to be a results of the effect on blood vessels by the tumour(s) [147] (see Chapter 23). Elastic�van Gieson staining reveals adventitial elastic sclerosis of both mesenteric arteries and veins, with luminal venous thrombosis. Ghosts of necrotic tumour cell islands (yellow) are seen among the perivascular fibrous tissue. The tumour cells are uniform, with little pleomorphism, nuclear hyperchromasia or mitotic activity. A new proposed grading scheme using mitotic count and Ki-67 index provides the potential of increased prognostic stratification (Table 24. Erosion of the serosal floor may result in solitary peritoneal deposits [148] or to a diffuse peritoneal carcinomatosis [149]. Involved lymph nodes may turn out to be large, measuring as much as 60 mm in diameter, and are frequently considerably larger than the primary tumour in the bowel wall. By far the most common website for distant metastases is the liver, the proper lobe being involved extra typically than the left. The incidence varies greatly in several published series, partly relying on the proportion of symptomatic instances studied [140] however is said to the dimensions of the first tumour. In one series, 53% of tumours measuring more than 20 mm had liver metastases compared with 20% of smaller tumours [157]. On the other hand, very small (5 mm) primaries can be accompanied by liver metastases. Metastatic illness to locations apart from the regional lymph nodes and the liver are uncommon however embody the ovary, spleen, pleura, heart, breast, skin, uveal tract, cervical lymph nodes and bone marrow [140,158,159]. The syndrome consists of episodic cutaneous flushing of the face and neck, sweating, diarrhoea, wheezing and hypotension. Right-sided heart illness could develop, because of fibrosis/plaques of the ventricular surface of the tricuspid valve, the pulmonary arterial floor of the pulmonary valve and the subendocardium of the best aspect of the guts [150]. The frequency of carcinoid coronary heart disease has markedly diminished, in all probability secondary to the utilization of somatostatin analogues [154]. Approximately two-thirds also stain for carcinoembryonic antigen and about 20% for prostatic acid phosphatase (but not prostatic-specific antigen) [140]. Of notice, cdx-2 is constructive in midgut carcinoids and may be helpful in assigning a primary web site in instances of an unknown primary [153]. It will not be localised around the primary tumour and may simulate a desmoplastic response to tumour, leading to mesenteric fibrosis (so-called frozen mesenteric root) and intestinal obstruction. Fibrosis could prolong to contain different organs together with lungs, skin or cardiac valves [154]. Even in patients with distant metastases, a 5-year survival of 40% compares favourably with the 5% for adenocarcinoma [28]. Overall, the 5-year consequence is also higher for ileal tumours (71%) than for jejunal neoplasms [49%]. Features reported to be of prognostic significance embrace tumour size, depth of invasion in to the bowel wall [161], metastatic illness on the time of surgery, a mitotic rate of greater than 4 mitoses per 50 hpf and the presence of the carcinoid syndrome. The last three had been discovered to have independent significance in a multivariate analysis of 167 circumstances [140]. In that research no patient with an preliminary tumour <10 mm in diameter, or with no nodal or liver metastases at the time of diagnosis, died of illness. Other antagonistic prognostic components embrace extra-abdominal unfold, substantial (>9 kg) weight reduction, intestinal ischaemia and carcinoid valvular coronary heart illness [160].
Buy actonel in united states online. Flu Symptoms And Treatment - Home Made Remedy Natural Tips For Flu Treatment - Any Body Used It.
References
- Bostom AG, Rosenberg IH, Silbershatz H, et al. Nonfasting plasma total homocysteine levels and stroke incidence in elderly persons: the Framingham Study. Ann Intern Med 1999;131:352-5.
- Yamada T, Sawaki Y, Tohnai I, et al. A study of sports-related mandibular angle fracture: relation to the position of the third molars. Scand J Med Sci Sports 1998;8:116-119.
- Gupta, N.P., Kumar, A. Analgesia for pain control during extracorporeal shock wave lithotripsy: current status: Indian J Urol 2008;24:155-158.
- Fujino M, et al. Disappearance of epidermal growth factor receptor is essential in the fusion of the nasal epithelium. Anat Sci Int 2003;78:25-35.
- Hochhaus A, Saglio G, Larson RA, et al. Nilotinib is associated with a reduced incidence of BCR-ABL mutations vs imatinib in patients with newly diagnosed chronic myeloid leukemia in chronic phase. Blood 2013;121(18):3703-3708.
- Aversa SM, Cattelan AM, Salvagno L, et al: Chemo-immunotherapy of advanced AIDS-related Kaposiis sarcoma, Tumori 85:54n59, 1999.
- O'Leary MP, Lue TF: Penile function. In Sant GR, editor: Pathophysiologic principles of urology, Blackwell, 1994, Oxford, pp 181-207.
- Vermorken JB, Remenar E, van Herpen C, Gorlia T, Mesia R, Degardin M, et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med 2007;357(17):1695-1704.